Dear Editor,
I am writing to emphasise the critical significance of laser treatment in physical therapy practice and to address a notable gap in current knowledge on high-intensity laser therapy (HiLT) dosing. Laser therapy is a non-invasive treatment widely used by physical therapists for its effectiveness in pain management, inflammation control, tissue repair, and muscle performance enhancement [1–5]. indeed, a substantial body of evidence supports its use in musculoskeletal pain management, further reinforcing its importance in the field [2, 3].
Lasers are classified into low-level laser therapy (LLLT) and HiLT, primarily determined by their power output [4]. LLLT emits at lower power levels (less than 0.5 W) and relies on photobiomodulation for its effects [2, 3]. in contrast, HiLT, uses higher power levels (0.5 W or more) and combines tissue heating with photobiomodulation effects. Furthermore, HiLT employs longer wavelengths that enable deeper tissue penetration compared to LLLT [5].
While LLLT has established dosing recommendations, proposed by the World Association for Photobiomodulation Therapy (WALT), for pain management in various musculo-skeletal disorders (https://waltpbm.org/) [6–8], HiLT is a relatively recent resource that has yet to receive widespread dissemination. As such, HiLT currently lacks a standardised dosage guide or recommendations for clinical use or research. To address this knowledge gap and support physical therapist practitioners, this letter presents a compilation of HiLT dosage suggestions for managing musculoskeletal disorders, sourced from various systematic reviews (SRs) and meta-analyses (MT-A).
An electronic search for SRs related to HiLT in musculo-skeletal conditions was conducted across the PubMed, Scopus, Web of Science, CiNAHL, and Cochrane library databases, with the last update on February 19, 2025. Keywords were obtained from the Medical Subject Headings (MeSH) vocabulary, used for article indexing in PubMed, and used to create search terms. The search terms included “Lasers,” “Laser Therapy,” “Phototherapy,” “High-Intensity Laser Therapy,” “Class IV laser,” “Musculoskeletal Pain,” “Neck Pain,” “Myofascial Pain Syndromes,” “Low Back Pain,” and “Pain Management.” These keywords were combined using Boolean connectors “oR” and “ANd” to create an effective search algorithm: ((“Lasers” OR “Laser Therapy”) OR (“Phototherapy”) OR (“High-Intensity Laser Therapy”) OR (“Class IV laser”) AND (“Neck Pain”) OR (“Musculoskeletal Pain”) OR (“Myofascial Pain Syndromes”) OR (“Low Back Pain”) OR (“Pain Management”)). Specific filters, including “Clinical Trial,” “Randomized Controlled Trial,” “systematic review,” and “meta-analysis,” were applied to obtain relevant results.
The inclusion criteria encompassed SRs and studies that involved participants experiencing musculoskeletal pain. The treatments considered were those using HiLT (Class iV or high-power lasers), either as standalone interventions or in combination with other treatments. These interventions were compared to other therapies, including physical therapy and medical treatments, or placebos, with the primary outcome measurement centered on pain intensity.
Exclusion criteria comprised case studies, literature reviews, scoping reviews, and other SRs specifically focused on HiLT in non-musculoskeletal disorders. Additionally, studies involving participants with neurological conditions were excluded. Furthermore, studies with incomplete or unavailable texts were excluded.
Results
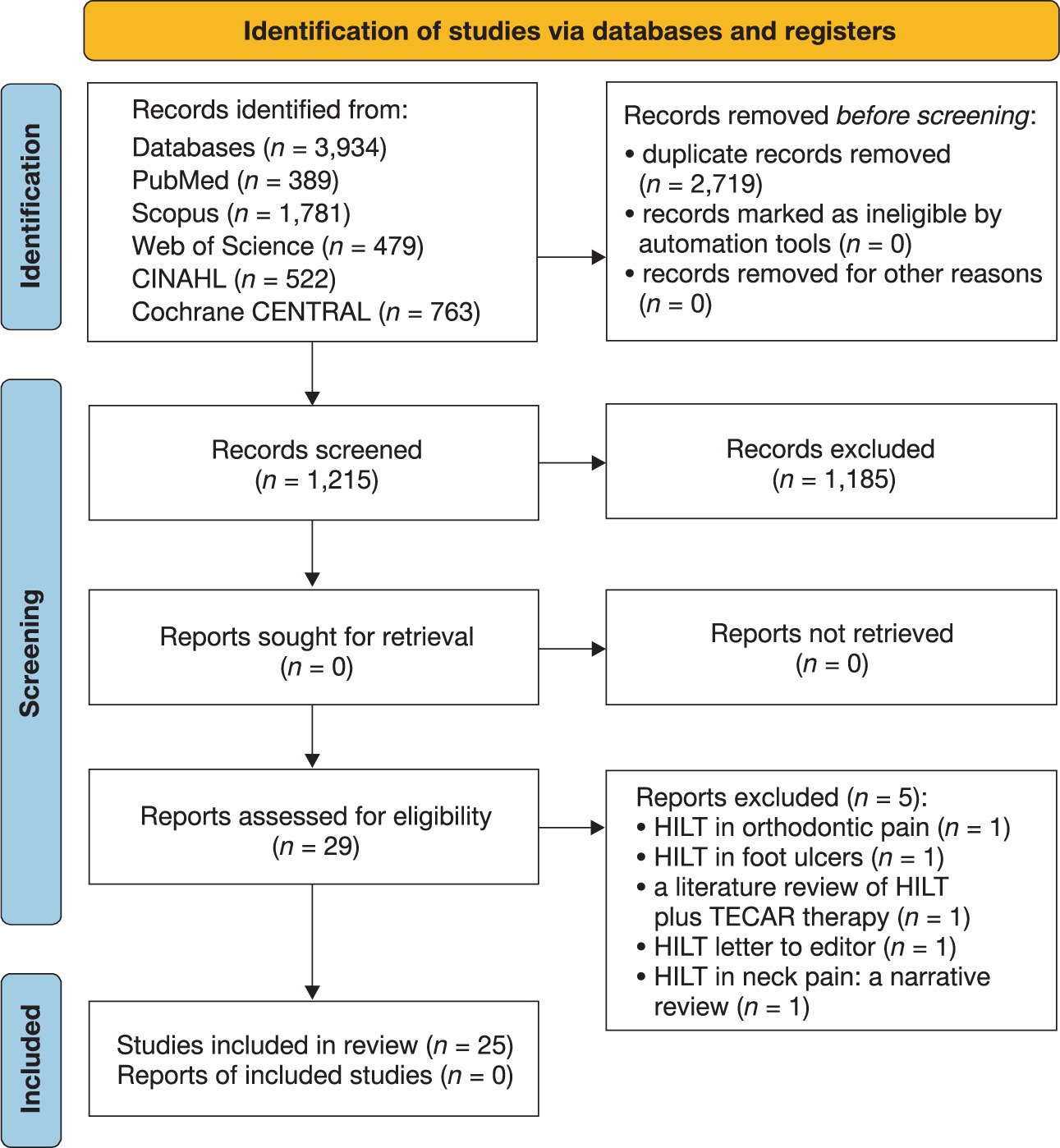
The initial search identified 3,934 articles (Table 1), with 1,215 subject to further analysis after removing duplicates. Subsequently, the titles and abstracts of these studies were reviewed, resulting in the selection of 30 studies. Five studies were excluded as they did not align with the focus on musculoskeletal conditions. These studies delved into areas unrelated to the subject matter, specifically HiLT for orthodontic pain, HiLT for foot ulcers, a literature review on HiLT combined with capacitive and resistive electric transfer (TECAR) therapy, a literature review on HiLT for neck pain, and a letter to the editor [9–13]. Therefore, a total of 25 SRs were obtained [4, 14–37]. Figure 1 depicts the PRiSMA flowchart delineating the search strategy and article selection.
Table 1
Results for the keywords, with and without Boolean connectors, employed in the search strategy across the electronic databases reviewed (last updated on February 19, 2025)
The SRs were conducted between 2018 and 2025 and focused on applying HiLT to pain management in various conditions, including general musculoskeletal pain [4, 15, 18, 21, 24, 26], myofascial pain [20], frozen shoulder [27], lateral epicondylalgia [19, 29, 31], knee osteoarthritis [14, 17, 22, 25], temporomandibular pain [32, 34], spinal disorders [16, 23, 30, 33], plantar fasciitis [28], carpal tunnel syndrome [36], and de Quervain’s tenosynovitis [37]. Eighteen SRs included MT-A [15–22, 22, 23, 25–37]. The most relevant outcomes were related to pain intensity and disability.
The data extraction for establishing dose recommendations was developed by analysing the clinical trials grouped within the SRs for each specific condition. Relevant parameters, such as emission mode, application technique, average power (W), treatment area (cm2), total delivered energy (J), and site of application, were considered. Consider that the treatment duration will vary according to the mean output power and the desired energy delivery: treatment time (s) equals energy (J) divided by mean power (W).
These recommendations are intended to provide initial guidance and are presented below for 1064 nm Neodymium-doped Yttrium Aluminum Garnet (Nd:YAG) lasers, the most commonly used lasers in this therapeutic context (Table 2).
Table 2
Suggested treatment doses for HiLT using 1,064 nm wavelength Neodymium-doped Yttrium Aluminium Garnet (Nd:YAG) lasers with a mean output of 1–20 W, an average spot size of 3.14 cm2, and a 30 mm spacer
| Musculoskeletal disorder | Treatment | Emission mode | Technique | Mean power (W) | Area/points | Energy (joules) | Application |
|---|---|---|---|---|---|---|---|
| Temporomandibular disorders [32, 34] | 3 phases | phase 1: pulsed phase 2: pulsed phase 3: continuous | phase 1: quick scan phase 2: punctual phase 3: slow scan | phase 1: 10.5 W phase 2: 10.5 W phase 3: 10.5 W | phase 1: 25cm2 phase 2: at least 5 points phase 3: 25 cm2 | phase 1: 498 J phase 2: 6–7.8 J/point phase 3: 498 J | mandibular branch (scan); masseter/temporal muscles (punctual) |
| Myofascial pain [20] | 3 phases | phase 1: pulsed phase 2: pulsed phase 3: continuous | phase 1: quick scan phase 2: punctual phase 3: slow scan | phase 1: 3 W phase 2: 3 W phase 3: 8 W | phase 1: 25cm2 phase 2: at least 3 points phase 3: 25 cm2 | phase 1: 500 J phase 2: 10–15 J/point phase 3: 500 J | upper trapezius muscle |
| Chronic neck pain [16, 23, 33] | 3 phases | phase 1: continuous phase 2: pulsed phase 3: continuous | phase 1: quick scan phase 2: punctual phase 3: slow scan | phase 1: 3 W phase 2: 3 W phase 3: 8 W | phase 1: 25cm2 phase 2: at least 3 points phase 3: 25 cm2 | phase 1: 1,025 J phase 2: 25 J/point phase 3: 1,025 J | cervical tracts and repeat dose for upper trapezius muscle |
| Cervical spondylosis [16, 23, 33] | 3 phases | phase 1: continuous phase 2: pulsed phase 3: continuous | phase 1: quick scan phase 2: punctual phase 3: slow scan | phase 1: 3 W phase 2: 3 W phase 3: 7 W | phase 1: 50 cm2 phase 2: at least 8 points phase 3: 50 cm2 | phase 1: 1,000 J phase 2: 25 J/point phase 3: 1,000 J | upper trapezius muscle and cervical tract (C4-T4) |
| Cervical radiculopathy [16, 23, 33] | 3 phases | phase 1: continuous phase 2: pulsed phase 3: continuous | phase 1: quick scan phase 2: punctual phase 3: slow scan | phase 1: 3 W phase 2: 3 W phase 3: 8 W | phase 1: 25 cm2 Phase 2: at least 3 points phase 3: 25 cm2 | phase 1: 625 J phase 2: 33 J/point phase 3: 625 J | same application for the cervical spine, upper trapezius, and interscapular region |
| Frozen shoulder [27] | 2 phases | phase 1: pulsed phase 2: continuous | phase 1: quick scan phase 2: slow scan | phase 1: 8 W phase 2: 8–12 W | phase 1: 25 cm2 phase 2: 25 cm2 | phase 1: 100–300 J phase 2: 100–300 J | anterior and posterior portions of the deltoid muscle (scan) |
| Subacromial impingement syndrome [4, 18, 35] | 3 phases | phase 1: continuous phase 2: pulsed phase 3: continuous | phase 1: quick scan phase 2: punctual phase 3: slow scan | phase 1: 8 W phase 2: 3 W phase 3: 12 W | phase 1: 25 cm2 phase 2: tender points phase 3: 25 cm2 | phase 1: 1,000 J phase 2: 50 J/point phase 3: 2,000 J | anterior and posterior portions of the deltoid muscle (scan); tender spots (punctual) |
| Lateral epicondylitis (tennis elbow) [19, 29, 31] | 2 phases | phase 1: pulsed phase 2: continuous | phase 1: punctual phase 2: scan | phase 1: 4–6 W phase 2: 8 W | phase 1: 1–2 points phase 2: 25 cm2 | phase 1: 6 J/point phase 2: 675 J | lateral epicondyle (punctual); forearm extensor muscles (scan) |
| Carpal tunnel syndrome [36] | 3 phases | phase 1 and 2: pulsed phase 3: pulsed | phase 1: fast scanning phase 2: punctual on trigger points phase 3: slow scanning | phase 1 and 2: 8 W phase 3: 7 W | phase 1: 25 cm2 phase 2: tender points phase 3: 25 cm2 | phase 1 = 647 J Phase 2 = 648 J phase 3 = 1,000 J | punctual on the flexor retinaculum and median nerve course |
| Low back pain [16, 30] | 3 phases | phase 1: continuous phase 2: pulsed phase 3: continuous | phase 1: fast scanning phase 2: punctual on trigger points phase 3: slow scanning | phase 1: 3 W phase 2: 3 W phase 3: 3 W | phase 1: 50 cm2 phase 2: tender points phase 3: 50 cm2 | phase 1 = 1,400 J phase 2 = 200 J (25 J for each point) phase 3 = 1,400 J | transversally along the low back; bilaterally at eight paravertebral points from L1 to S3 |
| Knee osteoarthritis [14, 17, 22, 25] | 1 phase | phase 1: pulsed phase 2: continuous | phase 1: quick scan phase 2: slow scan | phase 1: 10.5W phase 2: 5 W | phase 1: tender spots phase 2: 25 cm2 | phase 1: 15-60 J/cm2 phase 2: 2,400–3,000 J | medial and lateral sides of the knee surface (scan) |
| Plantar fasciitis [28] | 1 phase | continuous | slow scan | 12 W | 25 cm2 | 3,000 J | cover the entire sole of the foot (scan) |
| de Quervain’s tenosynovitis [37] | 2 phases | phase 1: pulsed phase 2: continuous | phase 1: punctual phase 2: scan | 8 W | phase 1: tender spots phase 2: 25 cm2 | phase 1: 80 J phase 2: 1,250 J | punctual application on the first extensor compartment and scanning the wrist and the dorsal forearm |
The recommendations are based on an analysis of parameters that have demonstrated a high frequency or are frequently reiterated in related studies and are dependent on changes in pain assessment intensity using the Visual Analog Scale (VAS) [38]. All reviews with meta-analysis consistently demonstrated significant statistical changes in favour of HiLT compared to control groups, placebos, and other interventions, with a pooled effect in terms of mean differences (Md) for VAS ranging from –0.9 cm to –3.0 cm, or a standard mean difference (SMd) between 0.5 and 1.0 that represents a high effect size in favour of HiLT-treated groups [15–23, 25–37]. These values are mostly close to or exceed the clinically minimal important difference (MCid) reported for VAS, which is around –1.3 cm (Ci 95 %: 1.1,1.7) [38, 39].
Conclusions
Laser therapy, comprising LLLT and HiLT, is a commonly employed therapeutic modality by physical therapists for addressing pain in different musculoskeletal disorders. it is crucial to recognise the emerging significance of HiLT and its evolving dosage recommendations to foster a comprehensive understanding and effective use of this resource in musculo-skeletal disorder pain management.
The analgesic effects of HiLT vary depending on the specific musculoskeletal condition being addressed, with pronounced analgesia notably observed in temporomandibular pain and musculoskeletal conditions involving the shoulder, elbow, and wrist. Conversely, SRs reported that HiLT use is less clear in cases related to foot conditions. However, it is crucial to highlight the limitations related to the number of studies addressing each specific condition and the substantial heterogeneity (I2 index) reported in the MT-A, which may lead to potential underestimation or overestimation of the results regarding analgesia, emphasising the imperative need for further research on the effects of HiLT in these conditions and others. Additionally, the quality of many of the reviews has been evaluated using AMSTAR-2 (A Measurement Tool to Assess Systematic Reviews), which generally identifies several methodological deficiencies [40].
Although a generally positive analgesic response to laser therapy is observed across various musculoskeletal disorders, it is imperative to acknowledge that the degree of analgesia may be influenced by several factors. These factors encompass the type of tissue undergoing treatment (considering the number of chromophores), the stage of the healing process within the damaged area, the synergy of nonthermal (solely photobiomodulation) and/or thermal effects of the laser employing different pain-relieving mechanisms, and the number and frequency of treatment sessions. Consequently, these dosage recommendations intend to serve as an initial approximation for future RCTs and clinical applications. As such, there remains the possibility of refinement based on new evidence as it becomes available.