Introduction
Ageing is a natural phenomenon [1]. It starts from the day of birth and ends with the cessation of life. Senescence is a hallmark of ageing [2]. Senescence affects all body systems, causing up to a 3% loss of function annually in 13 systems between the ages of 30 and 70 [3]. This process is accompanied by a decline in the physical function of an organism and an increase in age-related chronic diseases [4, 5]. Declining function, the prevalence of chronic disease, and associated medication increase the risk of falling [6].
In 2012, the proportion of older adults (over 60) in Sri Lanka was 12.4%. It is forecast that the percentage will be 25% by 2041 [7] and 35.6% by 2100 [8]. The term ‘fall’ is defined as the unintentional act of coming to a rest on the ground, floor, or any lower level, specifically excluding deliberate changes in position to rest on furniture, walls, or other objects [9]. The World Health Organization has identified falls among older adults as a global health problem, and falls are likely to emerge as a significant public health problem in Sri Lanka [10].
The prevalence of falls varies according to region. Every year, more than 30% of older adults aged 65 and above experience falls [6]. Falls can be caused by a combination of factors and also interaction among those factors [11]. The risk factors for falls can be classified in different ways. One classification categorises the risk factors as intrinsic and extrinsic. Intrinsic factors are patient-related and include age, sex, neurological and musculoskeletal issues, as well as visual, auditory, endocrine, gastrointestinal, genitourinary, and cardiovascular factors. Extrinsic factors, on the other hand, are environmental factors external to the patient. Cardiovascular risk factors for falls include arrhythmias such as atrial fibrillation (AF), postural hypotensive syncope, thyroid disorders, dyslipidemia, a history of acute myocardial infarction, previous stroke, systemic arterial hypertension [12], heart failure, and type 2 diabetes mellitus [13]. The neurological causes of falls may include age-related changes in the central nervous system and sensory system, and disease conditions associated with the nervous system [14]. The environmental factors contributing to increased fall risks are poor flooring, poorly designed bathtubs, poorly arranged furniture, inadequate lighting, and obstructed walkways [15]. Few studies have been conducted in Sri Lanka on falls among older adults [16, 17], and no systematic literature review has been conducted yet. Therefore, the objective of this study was to synthesise the literature related to the prevalence, epidemiology, and fall prevention programmes implemented to reduce falls among older adults in Sri Lanka.
Subjects and methods
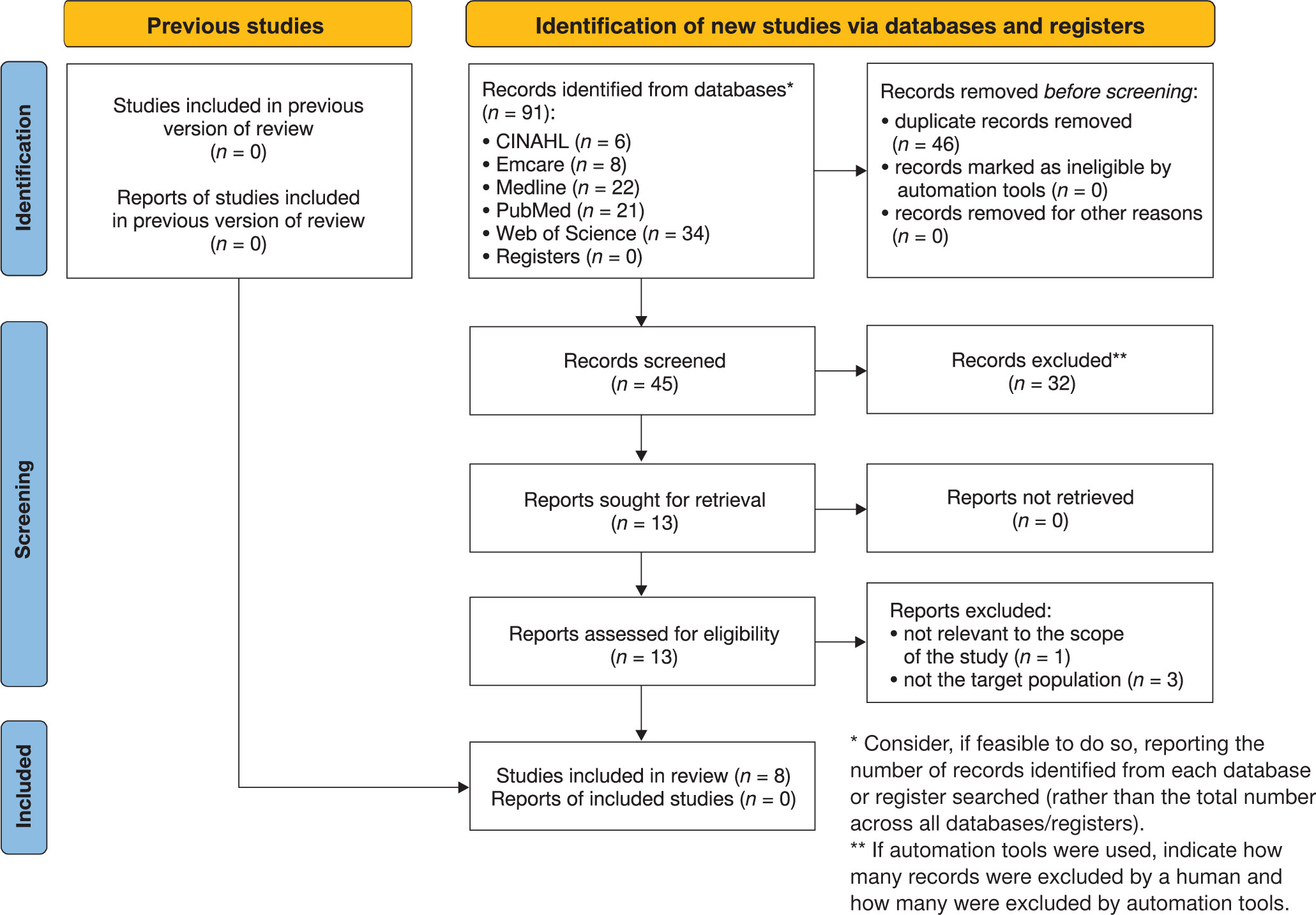
The scoping review was conducted according to the guidelines provided by the Joanna Briggs Institute (JBI) for scoping systematic reviews [18] and Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (Annexure-1) [19]. The references identified through the searches were exported to Rayyan, and duplicates were removed. Title, abstract, and full-text screening were performed by two independent reviewers (I.L. and E. L.), and data extraction was also independent of the same reviewers. Any disagreement between the two reviewers was resolved with the involvement of a third reviewer (K.G.). The (PRISMA-ScR) [20] flow diagram is shown in Figure 1. This scoping review was registered with Open-Science Framework (osf.io/dqps2).
Objectives and research questions
The aim of this study was to achieve the following objectives: First, to describe how commonly falls occur among older adults in Sri Lanka. Second, to identify and summarise the risk factors that contribute to falls among older Sri Lankan adults. Third, to identify and summarise information about fall screening, assessment of fall-related parameters, and fall prevention programmes developed to reduce the risk of falls among older adults in Sri Lanka.
Inclusion and exclusion criteria
The research questions were formed by following the JBI and the PCC framework (population, concept, and context) [21], with older adults over 60 years of age living in Sri Lanka taken as the population, falls among older adults in communities and institutions as the concept, and Sri Lanka as the context. All articles encompassing research studies published in English and carried out within the geographical confines of Sri Lanka were incorporated. Articles that were not accessible in English were excluded. The assessment encompassed studies focusing on the incidence of falls among older individuals residing in the community with an age of 60 years or older.
Database search
The methodology employed in the exploration of the literature for the scoping review adhered to the identical three-step process advised in traditional JBI systematic reviews [22]. The databases that were examined included Web of Science, PubMed, MEDLINE, Emcare, and CINAHL via the EBSCOHost® platform, and the following keywords were used: ‘older adult*’, ‘older people’, ‘elderly’, ‘senior*’, ‘geriatric’, ‘fall*’, ‘accidental fall*’, and ‘Sri Lanka’. Articles published up to the 22nd of May 2024 were included.
Results
A total of 91 studies were identified through a thorough exploration of the selected databases (Figure 1) after redundant entries were eliminated. Following the application of the predetermined inclusion criteria, nine studies met the requirements for inclusion in the comprehensive analysis. All studies under consideration were observational in nature, with a conspicuous absence of review or interventional studies.
Prevalence of falls among older adults in Sri Lanka
Five studies examined the prevalence of falls among older adults in Sri Lanka. The prevalence varies from 47.1% to 52% in institutionalised older adults, and among community-dwelling older adults it varies from 23% to 34.3%. Most studies were conducted in Colombo, the capital city of Sri Lanka, Galle, the capital city of the southern province, and Kandy, the capital city of the central province. Table 1 summarises the prevalence of falls among older adults in Sri Lanka.
Table 1
Prevalence of falls among older adults in Sri Lanka
| Author | Type of study | Setting | Prevalence of falls |
|---|---|---|---|
| Gamage et al. [23] | cross-sectional study | community-dwelling, Galle district | 34.3% |
| Ranaweera et al. [16] | cross-sectional nested case-control study | community-dwelling, Colombo district | 38.4% |
| Thanthrige et al. [24] | cross-sectional | institutionalised older adults, Colombo district | 52% |
| Weerasuriya and Jayasinghe [25] | cross-sectional study | hospital-admitted patients, Colombo district | 23% |
| Ihalage et al. [17] | cross-sectional study | institutionalised older adults, Kandy district | 47.1% |
Table 2
Risk factors associated with falls among older adults in Sri Lanka
| Author | Type of study | Setting | Risk factors for falls | Factors not associated with falls |
|---|---|---|---|---|
| Gamage et al. [23] | cross-sectional study | community-dwelling | age, sex, diabetes mellitus, balance or gait problems, use of antihypertensive medication, use of at least one long-term medication | environmental and socioeconomic factors |
| Ranaweera et al. [16] | nested case-control | community-dwelling | falls in the previous year, high disability level, high house risk levels | age, sex, ethnicity, education level, living arrangement, marital status, foot disorders, vision, cognitive status, presence of more than two chronic diseases, dizziness, mobility level |
| Thanthrige et al. [24] | cross-sectional study | institutionalised older adults with cognitive impairment | fall risk associated with balance, lower limb strength, cognitive function | not assessed |
| Wijerathna et al. [26] | cross-sectional study | patients admitted to hospital | age > 74 years, use of long-term multiple medications, fear of falling, cognitive impairment, depression, high-risk mobility, postural hypotension, reduced visual acuity | not assessed |
| Ihalage et al. [17] | cross-sectional study | institutionalised older adults | higher BMI, lower cardiovascular endurance, and lower flexibility in the lower body | body fat percentage, hand grip strength, lower body muscle strength and endurance, upper body flexibility |
Table 3
Tools used to assess fall-related parameters and fall prevention programme
| Author | Year | Type of study | Balance assessment tool | Strength assessment tool | Gait assessment tool | Falls | Fall screening tool |
|---|---|---|---|---|---|---|---|
| Gamage et al. [23] | 2019 | cross-sectional study | self-rated balance problem | not used | self-rated gait problem | falls in last year | not been used |
| Ranaweera et al. [16] | 2013 | nested case-control | TUG | not used | TUG | falls in last year | not been used |
| Wickramarachchi et al. [27] | 2023 | cross-sectional study | four-stage balance test | handgrip strength for upper limb 30-second chair stand test for lower limb | stand up and go test | not used | hand grip strength and lower limb strength |
| Thanthrige et al. [24] | 2014 | cross-sectional study | FTSST | FTSST | not used | TUG | not used |
| Ihalage et al. [17] | 2024 | cross-sectional study | not used | handgrip strength for upper limb 30-second chair stand test for lower limb | not used | falls in last year | not used |
Risk factors associated with falls among older adults in Sri Lanka
Five studies investigated the risk factors associated with falls among older adults. The risk factors that were identified bore similarities to those documented in other research studies; nevertheless, the findings displayed inconsistencies across the various studies. This discrepancy could be attributed to certain studies neglecting to assess all conceivable risk factors, thereby complicating the acquisition of a comprehensive risk profile. Two studies identified age and long-term medication use as risk factors [23, 26]. Table 2 summarises the risk factors associated and not associated with falls.
Tools used to assess fall-related parameters and fall prevention programme
The tools utilised in the studies were classified into the following categories: balance, strength, gait, and fall screening. Researchers categorised older adults into fallers and nonfallers based on the frequency of falls they experienced in the preceding year [16, 17, 23]. The Timed Up and Go test (TUG) is used to assess balance [16] and gait [27] and to categorise individuals as fallers or non-fallers [24]. Table 3 summarises the tools used and their respective roles in assessing falls in older adults.
Discussion
The global prevalence of falls varies from 20% to 33% [28]. A similar rate has been reported among community-dwelling older adults in Sri Lanka. However, a lower prevalence was reported among older adults in Japan (9% among males and 19% among females) [29], China (11%), and Malaysia (4%) [30]. This may be due to cultural differences between countries that affect activity levels, food habits, and environmental factors. A higher prevalence of falls has been reported among institutionalised older adults than among community-dwelling older adults in Sri Lanka. This is similar to studies conducted in other parts of the world, where institutionalised older adults report higher fall prevalences than their community-dwelling counterparts [31,32]. This high prevalence is due to the psychological impact of separation from the family [33] and a lack of physical activity when they are institutionalised [34].
Risk factors associated with falls among older adults
The identified risk factors were similar to those reported in other studies; however, the results were not consistent across all studies. This may be due to the fact that some studies did not evaluate all potential risk factors, which makes it difficult to obtain a complete risk profile.
The prevalence of falls increases with age, with 28% to 35% of those over 60 and 32% to 42% of those over 70 experiencing falls [9], making age a known risk factor. Many studies in developed countries have identified age as a risk factor [35]. However, one Sri Lankan study did not identify age as a risk factor [16], while the others did identify age as a risk factor [23, 26]. Similar inconsistent results have been reported for Saudi Arabia [36, 37]. This may be related to unmeasured biological, social, or environmental characteristics [36].
Sex has been identified as a fall risk factor, with females experiencing more falls than males [38]. This disparity may be due to underlying pathological conditions such as lower bone density and lifestyle factors after menopause [39, 40]. Similar results were reported by one researcher, who stated that females tend to fall more than males in Sri Lanka [23], but others did not identify sex as a risk factor. Similar results have been identified in Germany, where the fall rate among males increases with age, but not among females [41]. This may be due to the multifactorial nature of falls.
According to the literature, multiple medications increase the fall risk if more than four [42]. Studies in Sri Lanka have reported similar results [23, 26]. Multiple medications can cause adverse reactions that affect balance and cognition in older adults, increasing their vulnerability to falls [43]. It is also believed that reduced metabolic capacity with advancing age reduces the elimination of drugs, leading to an increased fall risk [44].
Older adults with one or more chronic conditions tend to experience more falls [45]. Inconsistent results have been reported in Sri Lankans regarding chronic health conditions and falls. Older adults in Sri Lanka are more likely to experience falls if they have certain chronic health conditions such as hypertension, diabetes mellitus, arthritis, or ischemic heart disease. Additionally, depression and cognitive impairment have been associated with an increased risk of falls in older adults in Sri Lanka. These chronic conditions can lead to disability and an increased risk of falls [44, 46, 47], but [16] reported that chronic conditions were not associated with falls.
Educational status has also been associated with falls among older adults [48]. Older adults with higher education levels experience fewer falls, as their education increases their awareness of falls [49]. However, inconsistent results have been reported in the literature [50], similar to those of the Sri Lankan studies.
Balance deficits [51], gait abnormalities, and lower limb weakness [52] are commonly associated with falls. The Sri Lankan studies are also consistent with this finding, except for one study, in which mobility was not associated with the risk of falls.
Tools used to assess falls-related parameters and fall prevention programmes
The American Geriatric Society and British Geriatric Society recommend initial screening and multifactorial assessment to identify older adults at risk of falling, as well as multifactorial interventions [53]. These screening tools are mainly based on questionnaires. Many countries have cross-culturally validated screening tools [54, 55]. Many Sri Lankan studies used the single question ‘Have you fallen during the period of the last twelve months?’ to identify falls among Sri Lankan older adults [16, 17, 23]. Balance, gait, and fall risk are commonly assessed by researchers using the TUG test [16, 24] and FTSST [24]. However, no reported studies used validated screening tools or multifactorial fall risk assessment to identify falls among older adults in Sri Lanka.
Conclusions
This scoping review provides information related to the prevalence, risk factors, assessment methods, and prevention of falls among older adults in Sri Lanka. All studies conducted in Sri Lanka were descriptive or analytical observational. No interventional studies have been conducted in this area. Studies related to falls have mainly been conducted in the Western, Central, and Southern provinces. Studies covering diverse older adult populations in other districts and sectors, such as the urban, rural, and estate sectors, are lacking. No study has been conducted in the estate sector, where 4% of older adults live in very different socioeconomic contexts. Potential reasons for falls in older adults in Sri Lanka consist of age, sex, medications, chronic conditions, education, balance deficits, gait abnormalities, and lower limb weakness. The results are inconsistent due to variations in the evaluated factors and unmeasured biological, social, or environmental characteristics. No validated fall prevention or screening programmes have been reported in Sri Lanka, highlighting the need for such programmes to address the ageing population.