Introduction
Joint hypermobility (JH) is the capability of one or more joints to move actively or passively beyond normal limits along physiological axes [1,2]. According to research conducted on a certain population, JH is prevalent at various degrees ranging from 5% to 40% in children and 10% to 20% in adults [3]. JH is usually ignored due to the absence of symptoms in all individuals, but failure to properly address this condition can lead to pain, injury, and joint arthritis [4–9].
JH is referred to as Local Joint Hypermobility (LJH) when only one or a few joints are observed to be hypermobile. It is also known as General Joint Hypermobility (GJH) when including five or more types of joints. Peripheral Joint Hypermobility (PJH) is the condition observed only in the hands and feet, while Joint Hypermobility Syndrome (JHS) describes the symptomatic cases. Joint instability, often found in only a few cases, is defined as insecurity of the joint to remain intact even under low-force conditions due to muscle, bone, and ligament loss in one or more movement planes [3]. JH can be acquired naturally through genetics, past trauma, joint disease, surgery, or training [2], with Ehlers-Danlos syndrome (EDS) being the most common type inherited genetically among other connective tissue disorders. EDS is an autosomal dominant trait marked by reduced serum levels of a large extracellular matrix glycoprotein known as tenascin-X. The lack of tenascin-X will significantly affect fragile tendons, septa, fascia, ligaments, and joint capsules [3]. Acquired JH may be inherited in the form of a normal trait with no identifiable genetic variant, as in EDS. However, the majority of JH is multifactorial, originating from a combination of environmental and genetic factors prone to muscle and ligament weakness or inflammation, which may perpetuate joint laxity [10]. Long-term training can cause adaptive changes and increase the range of motion (ROM), such as in athletes or dancers [11].
The Beighton Score (BS) is the most widely used method to determine JH, and is considered the gold standard, which consists of five standardised tests, including four bilateral, as shown in Figure 1 [12]. GJH is defined at a cut-off value of 3 6/9, 5/9, and 4/9 in children, individuals aged 50 years, and older adults, respectively [1]. According to previous research, JHS is commonly determined using the Brighton criteria [13], and the Villefranche criteria are applied for major EDS subtypes [14].
Figure 1
Beighton Scoring System to assess JH (used with permission from the Ehler-Danlos Society) [12]

JH is an advantage for individuals with professions demanding a greater ROM, such as dancers or gymnasts. This is associated with other symptoms, including fatigue, altered muscle activity, recurrent muscle sprains, reduced muscle strength, instability, and functional disability [15, 16]. Previous studies observed the physiological and pathological mechanisms of JH, then determined the type of training that could help affected individuals. Only a few found significant results, while the majority did not, leading to confusion regarding health interventions for JH individuals.
The ignorance about JH is challenging in society because certain healthcare systems often consider this condition as an advantage or provide the same treatments for symptomatic and asymptomatic individuals requiring special attention. Therefore, this study aimed to comprehensively review the assessment currently used to determine JH, health risk factors, and strategies for preventing future injuries in affected individuals. The review should increase awareness about the need for more efforts to prevent future chronic injuries capable of affecting the quality of life (QoL) among those with JH, irrespective of the benefits of being flexible.
Subjects and method
Study design
A scoping review was conducted to examine and analyse several existing studies following the method of Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews (PRISMA-ScR) [17]. The primary focus was on articles that observed JH in adolescents and adults over the past 11 years (2014–2024), but no methodological quality assessment was performed. This study was registered retrospectively in OSF Registries as Meiliana, A., Defi, I. R., Rosdianto, A. M., Tjitraresmi, A., Barliana, M.I. (October 4, 2024). Hypermobility: assessment, health risks, and prevention strategies – a scoping review. Retrieved from: osf.io/cm6yu with doi: 10.17605/OSF.IO/CM6YU.
Study selection
The population examined were adolescents and adults in the age ranges of 12–17 and 18–65 years old, respectively. Inclusion criteria were full-text studies concerning the effect of hypermobility on this population, as well as articles published in the English language from 2014 to 2024, and strategies to improve the health condition. Meanwhile, exclusion criteria comprised the presence of another disease influencing JH in subjects, non-investigative and qualitative research, as well as non-human research or review articles and those using secondary data. Updated database searching was conducted on August 22, 2024, across PubMed/Medline, Scopus, and CINAHL using standardised vocabulary consisting of Medical Subject Headings (MeSH), in combination with Boolean operators. Furthermore, the applied search terms included the title and abstract keyword ‘[tiab]’, as presented in Table 1.
Table 1
Search terms used in PubMed/Medline, Scopus, and CINAHL databases
Data analysis and synthesis
The review contexts and main results were charted based on PICOS (Population – Intervention – Comparison – Outcomes, and Study type) and broken down into (1) Authors and country where the research was conducted. (2) Population, including the number of subjects, age group, and type of hypermobility. (3) Measured variables comprising parameters used to assess hypermobility (GJH or JHS) and outcome parameters (muscle strength, pain, balance, injuries, recovery, fatigue, or QoL). (4) Comparison performed between groups or treatments, (5) Main results of each study, and (6) Conclusion. The tables (referred to Table 2–4) were presented based on the study type, while the population was grouped into trained (athletes or professionals) and untrained, as well as adolescents and adults to provide an overview of the two major factors influencing the degree of JH. Based on the chart, an analysis was conducted independently, then a group discussion was conducted until September 6, 2024, to determine the main problems faced by individuals with JH, and proposed clinical suggestions.
Results and discussion
Data extraction
The initial stage of this research was performed by one scientist, then a team of three members continued the other stages. A database search starting with PubMed was conducted using MeSH, including ‘joint hypermobility’, ‘joint instability’, ‘injury’, and ‘flexibility’ combined with boolean operators (‘AND’, ‘OR’) and ‘[tiab]’, followed by a manual search of references for selected studies.
The total number of studies found during the identification stage was 21,906, from which 369 were included for screening after removing some based on the range of publication year and duplication, with only 110 fulfilling the inclusion and exclusion criteria. Among the 73 that were eligible, 39 were irrelevant to the research questions due to not focusing on skeletal muscle injuries but other topics such as instrument development, and 36 were selected for final inclusion (Figure 2).
Demographic characteristics
The various types of reviewed studies were predominantly conducted in Europe, including 10 in the UK [4, 5, 8, 16, 18–23], six in Denmark [6, 9, 24–27], three in the Netherlands [29–31], and one in each of Poland [31], Switzerland [32], Italy [33], and Belgium [34]). Four were performed in the USA [35–38], three in Australia [9, 40, 41], two in the Middle East (specifically in Qatar [41] and Iran [42]), one in Brazil [15], one in China [7], and another one in Canada [43]. The number of subjects ranged from 21 to 1,584, which comprised both males and females. A total of 15 studies were conducted on trained subjects, namely five on adolescents [16, 24, 25, 41, 44] and 10 on adults [15, 18, 19, 29–32, 36, 39, 42], while 21 were performed on untrained subjects, including five on adolescents [6, 9, 28, 37, 45] and 16 on adults [4, 5, 7, 8, 20–23, 26, 27, 33–35, 38, 40, 43]. The majority (n = 18) were publicly funded, only two were privately funded, and the remainder (n = 16) did not state any funding source.
Figure 2
Overview of the study selection process (according to updated PRISMA-ScR on guidelines Equator.org)
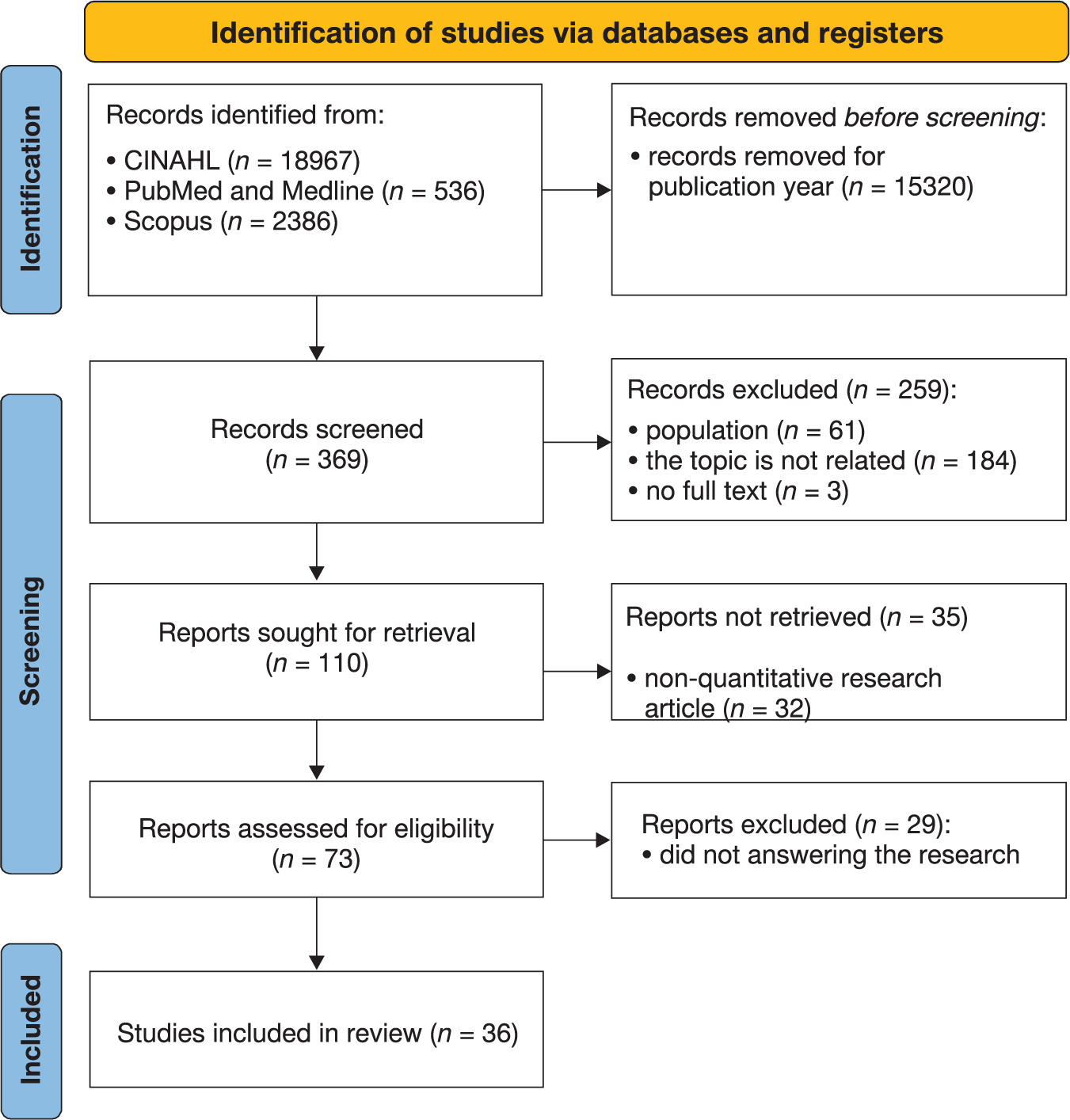
Table 2
Summary of the characteristics and main results of the cohort studies
| Authors (country) | Funding | Subject (population) | Measured variables | Comparison | Main results | Conclusion | |
|---|---|---|---|---|---|---|---|
| Trained adolescents | Vieira et al. (Brazil) [44] | N/A | 83 soccer players (14–19 y.o.) | – JFIS (Carter and Wilkinson) – episodes of ankle sprain – position in the team, affected side of the body, and moment of the trauma | JHSvs NF soccer players | – 22 subjects have JHS, while 66 as control. – A total of 43 cases of ankle injury due to sprains were recorded, of which nine episodes were in players with JHS, leading to p = 0.106. – There were increased ankle sprains in JHS but not significantly different. | There were no differences in the incidence of ankle sprain injuries between soccer players with JHS and non-JH counterparts. |
| Trained adults | Nicolay et al. (USA) [36] | private | 73 football players (7 GJH vs 66 NF) | – GJH (BS ≥4) – number of musculoskeletal issues, injuries, treatment episodes, days unavailable, and surgical procedures over two years | GJH vs NF | – During the two-year evaluation, there were 438 musculoskeletal issues, including 289 injuries. – Mean number of treatment episodes per athlete was 77 ± 71 (range, 0–340), and the mean number of unavailable periods was 67 ± 92 days (range, 0–432 days). – 23 athletes required 25 operations, with the most common procedure being arthroscopic shoulder stabilisation (n = 1/4 6). – Number of injuries per athlete was not significantly different between the GJH and no-GJH groups (3.0 ± 2.1 vs 4.1 ± 3.0; p = 1/4 0.13), nor were there any between-group differences in the number of treatments received (74.6 ± 81.9 vs 77.2 ± 71.5; p = 1/4 0.47), days unavailable (79.6 ± 124.5 vs 65.3 ± 89.3; p = 1/4 0.61), or rates of surgery (43% vs 30%; p = 1/4 0.67). – There was no greater risk of injury, but the number of games was nearly two times higher in players without GJH compared to those with GJH (11.6 ± 7.0 vs 6.1 ± 4.0; p = 1/4 0.008). | – There was no difference in injury numbers between GJH and non-GJH. – Number of games was higher in non-GJH. |
| Mayes et al. (Australia) [39] | N/A | 21 ballet dancers (18–39 y.o.) | – GJH (BS ≥ 5) – cartilage defects on hip 3T magnetic resonance imaging and pain (Copenhagen Hip and Groin Outcome Score: HAGOS) at baseline and follow-up, hip-related injury incidence, and retirement over 5 years | GJH vs NF | – Cartilage defect prevalence was lower in GJH (n = 1) than in non-GJH dancers (n = 17, p < 0.001). – BS ≥ 5 was predictive of cartilage defect presence at baseline, independent of age and gender (p = 0.006). – At follow-up, cartilage defects progressed in two dancers, featuring one hypermobile. – Baseline and follow-up HAGOS pain scores were similar in GJH and non-GJH dancers (p > 0.05 for all). – Hip-related injury over five years was reported by a similar number of GJH [n = 7) and non-GJH dancers (n = 6, p = 0.7). – Hypermobility was more prevalent in active dancers (n = 12) than retired dancers (n = 2), independent of age, rank, and gender (p = 0.03). – Hypermobile dancers were at no greater risk of reporting hip pain and injury or retirement over five years. | GJH was not considered a burden in professional ballet and may be an asset. | |
| Armstrong et al. (United Kingdom) [18] | N/A | 286 rugby, netball players, and dancers | – Beighton and Horan Joint Mobility Index (0–2 = not hypermobile; 3–4 = moderately hypermobile; 5–9 = distinctly hypermobile) – relative contribution of five joints to JH based on BS | male vs female subjects for each sport category | – Significant differences existed for group and gender analysis at the left and right fifth metacarpophalangeal joints, left and right thumb, left and right elbow, as well as lumbar spine (p < 0.001). – Female dancers had the highest prevalence (93%) of hypermobile lumbar flexion, which could be a sign of performance adaptation. | – Females and males were subject to differences in the relative contribution to JH. – The functional nature of lumbar flexion might require different interpretations in the BS. – Among female dancers, a positive lumbar flexion JH score might be a sign of performance adaptation compared to a measure of JH. | |
| Konopiński et al. (United Kingdom) [19] | public | 80 elite football players | – GJH (BS ≥ 4) – number of injuries – training days and matches missed due to injury | hypermobile vs non-hyper-mobile elite footballers | – Hypermobile players had a tendency for higher injury incidence, p = 0.06. – Training exposure was a significant risk factor for injury (p < 0.001) in elite football players with or without GJH. | – JH increased injury risk in elite footballers. – Medical staff should consider routine screening of footballers for JH. – Training exposure was found to be a significant injury risk factor for elite football players. | |
| Azma et al. (Iran) [42] | public | 721 soldiers | – BJHS (BS ≥ 4, 5 and 6) – prevalence of ankle sprain, shoulder, and TMJ dislocations | before vs after three months of military training (including endurance exercises, physical strength practices, and specific military education) | – Frequency of BJHS before military training was 29.4%. – After passing the military training period, the incidence of ankle sprain was significantly higher in the group with the BS ≥ 4 (4.3%, p = 0.03), 5 (5.5%, p = 0.005), and 6 (6.5%, p = 0.01) out of 9. – The incidence of temporomandibular joint dislocation was not significantly different based on the BS ≥ 4, but higher in the BS ≥ 5 (2.1%) and 6 (2.6%) for discrimination of two groups (p = 0.03). – There was no significant difference between the two groups in the case of shoulder dislocation. – Military training could increase the incidence of ankle sprains and TMJ dislocations in hypermobile individuals with a higher BS. | – Military training could increase the incidence of ankle sprains and TMJ dislocations in hypermobile individuals with a higher BS during training courses in comparison with non-GJH. – No differences in shoulder dislocation between all groups. | |
| Untrained adults | To and Alexander (United Kingdom) [22] | public | anterior knee pain physio patients (47 JHS, 29 GJH, and 26 NF) | – JHS (Brighton criteria), GJH (BS ≥ 4) – activity level – knee function (Lysholm scoring) – pain intensity (VAS) – pain killer used – muscle strength – teach, check, adapt, and progress exercise | individualised leg exercises, a cohort for 16 weeks | – JHS group had greater severity of pain (p = 0.00), poorer function (p = 0.00), and lower activity levels (p = 0.00). – There was no difference in the rate of change of concentric and eccentric muscle strength. – JHS was significantly weaker than the other two groups, taking three to four months to reach the baseline strength of the GJH group. – Subjects with JHS improved muscle strength at the same rate as other subjects. – Subjects started weaker, and many months were required to reach the starting strength of the peers with GJH. – Increase in strength was related to the decrease in pain. | Subjects with JHS could strengthen at the same rate as others in pain. |
| Luder et al. (Belgium) [34] | N/A | 51 GJH females | – GJH (BS ≥ 6) – muscle strength – muscle mass and density, functional activities, pain, and disability | 12-week resistance training twice weekly (experimental) vs no lifestyle change (control) | – JHS was determined using the Brighton criteria. – Mean strength of knee extensors varied in the training group from 0.63 (sd 0.16) N/bm before to 0.64 (SD =0.17) N/bm after training and in the control group from 0.53 (SD = 0.14) N/bm to 0.54 (SD = 0.15) N/bm. – There were no significant differences between groups. – There was no improvement in strength or muscle mass after 12 weeks of self-guided resistance training. | Improvement in strength or muscle mass by self-guided resistance training was not found. More individualised and better-guided training might be important. |
[i] BS – Beighton score, CL – Anterior Cruciate Ligament, EDSH – Ehler-Danhoss syndrome hypermobility, GJH – generalised joint hypermobility, HAGOS – Copenhagen Hip and Groin Outcome Score, HRQoL-Health-Related Quality of Life, JHS – joint hypermobility syndrome, LJH – local joint hypermobility, N/A – data not available, NF – normal flexibility, QoL – Quality of Life, TMJ – temporomandibular joint, VAS – Visual Analogue Scale, y.o. – years old
Table 3
Summary of the characteristics and main results of the cross-sectional studies
| Authors (country) | Funding | Subject (population) | Measured variables | Comparison | Main results | Conclusion | |
|---|---|---|---|---|---|---|---|
| Trained adolescents | Bukva et al. (Qatar [41] | N/A | 24 artistic gymnasts (11–26 y.o.) | – GJH (BS ≥ 5 for females and BS ≥ 4 for males) – years of training and weekly hours of practice – injuries (body part, mechanism, activity at the time of injury) – number of missed practices and competitions because of injuries | – correlation between JH scores to injury incidence – correlation between period of training to injury incidence | – The most commonly experienced injury was pain in the lower back, spine (25%), knee, hip, and ankle. – The injury was correlated with the total period of training than GJH. | – There was no correlation between GJH and injury rate. – Total training period had a greater contribution to the risk of injury. |
| Schmidt et al. (Denmark) [24] | N/A | 53 handball players, 57 gymnasts, and 22 ballet dancers (13–16 y.o.) Training exposures 6.5–10.5 hours/week | – prevalence of GJH (BS ≥ 4 and Brighton test) – FIRQoL and injury occurrence – Rheumatoid and Arthritis Outcome Score for Children (RAOS-Child) Version LK1.0 – static motor performance – dynamic motor performance | Subjects were classified based on three cut-off points: GJH4 for BS ≥ 4, GJH5 for BS ≥ 5, and GJH6 for BS ≥ 6 | –A higher prevalence of GJH4 was found in ballet dancers (68.2%) and gymnasts (24.6%) compared to team handball players 13.2%). – There was no significant difference in lower extremity function, injury prevalence, and related factors (exacerbation, recurrence, and absence from training). HRQoL, or dynamic motor performance tests were conducted for those with and without GJH. – GJH group had a significantly larger centre-of-pressure path length across sway tests in static motor performance, which increased the risk of ankle injuries. | Elite-level adolescent athletes in this study showed no difference in injury recurrence between the GJH or non-GJH groups, but GJH group had a higher risk of future injury. | |
| Trained adults | Blokland et al. (Netherland) [30] | N/A | 114 elite female soccer players | – GJH (BS ≥ 3, 4, and 5) – injury registration form (date of injury and recovery, type, location, time of sustaining injury (training/match), cause of injury by contact or collision (ie, with another player or ball), and specific diagnosis | subjects with BS < 3 vs BS ≥ 3, 4, and 5 | – 20 were classified as hypermobile (BS ≥ 4). – Mean (± SD) injury incidence/player was 8.40 ± 9.17 injuries/1,000 h of soccer, with no significant difference between hypermobile and non-hypermobile players. – GJH was not a risk factor for injuries when using BS cut-off points of ≥ 3 (IRR = 1.06 [95% Cl, 0.74–1.50]; p = 0.762), ≥ 4 (IRR = 1.10 [95% Cl, 0.72–1.68]; p = 0.662), or ≥ 5 (IRR = 1.15 [95% Cl, 0.68–1.95]; p = 0.602). – GJH was not a significant risk factor for thigh, knee, or ankle injuries evaluated separately. – Hypermobile players at this elite level might have improved their active stability and/or used braces to compensate for joint laxity. | – GJH was not considered a risk factor for injury in elite female soccer players. – Hypermobile players in this group of elite female soccer players might have improved active stability and/or used braces to compensate for JH. |
| Scheper et al. (Netherlands) [29] | N/A | 36 dancers and 36 nondancers | –GJH (BS ≥ 4) – functional status performance (self-reported physical activity level) and capacity [walking distance and jumping capacity, including side hop (SH) and square hop (SQH) – muscle strength – musculoskeletal complaints (pain and fatigue) | professional dancer vs non-dancer | – GJH was significantly higher among dancers (p = 0.001). – Subjects with GJH had a reduced walking distance (B(SE): –75.5(10.5), p = < 0.0001) and jumping capacity (SH : B(SE): –10.10(5.0), p = 0.048, and SQH: B (SE): –11.2(5.1), p = 0.024). – GJH was independently associated with lower walking and jumping capacity. – Pain, fatigue, and muscle strength were also important contributors to functional status. | GJH was independently associated with lower walking and jumping capacity, potentially due to the compromised structural integrity of connective tissue, which was majorly common in dancers. | |
| Sanches et al. (Brazil) [15] | public | 44 ballet students and 33 ballet teachers (18–40 y.o.) | – GJH, JHS (BS ≥ 4 and Brighton) – years of ballet; hours/week dancing | ballet teachers vs students | – Teachers had three times higher tendencies to have JHS than students (OR 3.02; 95% Cl 1.03–8.85), but there was no difference in GJH prevalence. – Dancers with JHS could engage in ballet teaching as an alternative to professional careers while maintaining less injury compared to those committed to dates, rehearsals, and performances, with less rest for recovery. | Teachers had three times higher tendencies to have JHS than students. | |
| Bascevan et al. (Switzerland) [32] | N/A | 47 healthy male athletes without knee injuries (23.48 ± 3.54 y.o.) | – degree of knee JH (goniometer) – isokinetic parameters of the leg musculature or H/Q ratio (Biodex System 4 isokinetic dynamometer) – anthropometric indices | with or without knee hyperextension (10° or more than full knee extension) | – Athletes with hyperextended knees had shorter legs (t-value = –2.23, p = 0.03, moderate ES) and shins (t = –2.64, p = 0.01, moderate ES). – Hypermobile athletes also had a lower H/Q ratio at an angular velocity of 60°/s (t = –2.11, p = 0.04 moderate ES) compared to those in the non-hyperextended group. – An increase in the H/Q ratio at an angular velocity of 60°/s was associated with the degree of knee JH (R = –0.29, p = 0.04). | – Athletes with knee JH had weaker hamstring strength and a lower H/Q strength ratio at lower angular velocities. – These results showed that targeted strength training programs for leg (i.e., hamstrings) muscles should help individuals with knee JH. | |
| Untrained adolescentsntr | Meulenbroek et al. (Netherlands) [28] | public | 11 adolescents with asymptomatic GJH, 51 controls (12–21 y.o.) | – asymptomatic GJH (BS ≥ 6 for < 18 y.o.; and BS ≥ 5 for > 18 y.o.) – perceived harmfulness (PHODA-youth) and muscle strength (dynamometry) – motor performance (Single-Leg-Hop-for-Distance) and physical activity level (PAL) (accelerometry) | GJH vs NF | – AGJH was associated with increased knee extensor muscle strength (peak torque/body weight; PT/BW), controlled for age and gender (dominant leg; β = 0.29; p = 0.02). – No other associations between asymptomatic GJH and muscle strength, motor performance, and PAL were found. – Perceived harmfulness was not more pronounced in adolescents with asymptomatic GJH. | Adolescents with asymptomatic GJH had increased knee extensor muscle strength compared to non-hypermobile controls. |
| Bettini et al. (USA) [37] | N/A | 40 adolescents with chronic pain and autonomic nervous system dysfunction | – JHS (BS ≥ 4 = JHS, BS ≥ 5 = HEDS) – pain threshold (neurometer) – written assessment for Central Sensitisation Inventory (CSI), Brief Pain Inventory, and Functional Disability Inventory | JH vs NF | – JH had a moderately significant correlation with central sensitisation measured by CSI, as well as increased pain sensitivity as evidenced by hypersensitivity of Aδ sensory nerve fibres. – The presence of central sensitisation was also positively associated with functional disability levels. – JHS was considered a potential antecedent to pain hypersensitivity and central sensitisation syndromes. | – JH was considered a potential antecedent to the development of central sensitisation and pain hypersensitivity. – Adolescents with JH had higher rates of comorbid chronic pain and functional disability. | |
| Morris et al. (Australia) [45] | public | 1,584 adolescents (14 y.o.) | –GJH (BS ≥ 4 and 6) – McCarron Assessment of neuromuscular Development (MAND) – frequency of moderate to vigorous exercises – socioeconomic status – musculoskeletal pain | GJH vs NF | – GJH was more common in females than males (60.6% vs 36.7%). – No association between pain area counts and GJH was identified using a cut-off of ≥ 4. – While using cut-off ≥ 6: both females (p = 0.025) and males (p = 0.01) showed significant associations between the number of pain areas and GJH, but the pain became worse with sports among males only (p = 0.002). | Appropriateness of using a BS cut-off to determine GJH should be re-assessed. | |
| Jensen et al. (Denmark) [9] | public | 16 females with GJ H and 11 controls | – GJH (BS ≥ 6) – EMG recording from knee flexor and extensor muscles | GJH vs NF | – Early rate of torque development was 53% faster for GJH. – Reduced hamstring muscle activation in females with GJH was found, while knee extensor and calf muscle activation did not differ between groups. – Flexion-extension and medial-lateral co-activation ratio during flexions were higher for females with GJH than those with NF. This was explained by decreased agonist drive to the hamstring. – Females with GJH had a higher capacity to rapidly generate force than those with NGJH, which might reflect motor adaptation to compensate for JH. | – Females with GJH had a higher capacity to rapidly generate force than females with NGJH, which might reflect motor adaptation to compensate for JH. – Higher medial muscle activation represented higher levels of medial knee joint compression in females with GJH. – Increased flexion-extension co-activation ratios in GJH were explained by decreased agonist drive to the hamstrings. | |
| Untrained adults | Bates et al. (United Kingdom) [4] | public | 23 adults with JHS, 23 GJH, and 22 NF | – JHS (Brighton criteria), and GJH (BS ≥ 4) – VAS score – Gait and stair-climbing performance – Temporal-spatial, sagittal plane, kinematic, and kinetic outcome measures were calculated, then input to statistical analyses by statistical parametric mapping (SPM) | JHS vs GJH vs NF | – VAS score (pain intensity): JHS > GJH and NF. GJH ~ NF. – Gait: length of NF and JHS (p < 0.001 in both cases). – JHS had significantly lower power (ankle and hip) compared to GJH and NF. – GJH group was equally as hypermobile as the JHS group, but only one significant difference was observed between the GJH and NF groups. – GJH individuals might use compensatory mechanisms to ‘overcome’ JH, which were probably not applied by affected individuals. | Individuals with JHS were applying a knee-strategy and avoiding the use of the ankle. Compensatory mechanisms were used among those with GJH to ‘overcome’, compared to individuals experiencing JHS. |
| Reuter (USA) [38] | public | 816 undergraduate students | – LJH (BS 1–4), GJH (BS ≥ 5) – self-reported musculoskeletal injuries | JHS vs GJH vs NF | – Athletically active subjects reported more musculoskeletal injuries than those who were not athletically active (OR = 3, p < 0.0001). – Females had lower rates of self-reported injuries than males (55.4% vs 65.5%; p 1/4 0.0099; odds ratio: 1.53). – Most commonly reported injury types for both females and males were quadriceps, groin, and hamstring injuries. – Those with GJH or LJH did not report higher rates of musculoskeletal injuries. | Athletically active subjects sustained a greater risk of injury than JH. | |
| Untrained adults | Zhong et al. (China) [7] | public | 489 college students | – GJH (BS ≥ 4) – International Physical Activity Questionnaire (IPAQ) – knee joint 6DOF kinematic data during treadmill gait | GJH vs NF | – GJH showed greater flexion after the terminal stance ( = 0.039) and greater anterior translation of the tibia during nearly the whole gait period than the normal group (p < 0.05) during the treadmill gait. – A greater external angle was found in the GJH group during periods of middle stance (p = 0.008). – Poor active motion stability in anterior/posterior translation might play an important role in the development of knee JH, potentially leading to subsequent ACL. – Deficiency and the development of knee osteoarthritis among i ndividuals with GJH. | The knee in active motion was also unstable in GJH, potentially leading to subsequent ACL deficiency and knee osteoarthritis development. |
| Krähe et al. (Australia) [40] | N/A | 117 adults with JHS, EDSH, or both | – JHS (Brighton criteria)/EDS-HT (Villefranche) – fatigue, QoL, mental health, physical activity participation, and sleep quality (questionnaire) | JHS/EDS-HT vs NF | – Significant fatigue was reported by 79.5% of the 117 subjects. – There was a significant correlation between fatigue and psychological symptoms such as depression, stress, and anxiety, thereby decreasing QoL. | JHS/EDS-HT experienced significant symptoms of fatigue. | |
| Bates et al. (United Kingdom) [21] | public | 23 adults with JHS, 23 GJH, and 22 NF | – JHS (Brighton criteria), GJH (BS ≥ 4) – fidgets and sways counted during a maximum of 15 min standing across two force-plates | JHS vs NF | – Mean standing time for those with JHS was 7.35 min and none stood for a full 15 min. – All subjects with GJH and NF completed 15 min of standing. – There were no differences in fidgeting behavior between any groups. – There was a difference in anteroposterior sway (p = 0.029) during quiet standing periods. | Increased anteroposterior-sway might suggest a muscle weakness. | |
| Juul-Kristensen et al. (Denmark) [26] | public | 1,006 adults | – GJH (BS ≥ 4), GJHS (BS ≥ 4 + shoulder hypermobility) – Five-Part Questionnaire for classification of GJH – Standardised Nordic Questionnaire for musculoskeletal symptoms – EuroQoL-5D for HRQoL | GJH vs NF | – Prevalence of GJH and GJHS were 30% (n = 300) and 5% (n = 51), respectively. – Compared with Non-GJH (NGJH), those with GJH and GJHS had an Odds Ratio (OR) of 1.5–3.5 for upper body musculoskeletal symptoms in the past 12 months (mostly shoulders and hands/wrists). – GJH and GJHS also had OR 1.6–4.4 for being prevented from usual activities, mostly due to shoulder and neck symptoms. – GJH and GJHS had OR 2.2–3.1 for upper body musculoskeletal symptoms ranging for more than 90 days (neck, shoulders, hand/wrists), and 1.5–3.5 for reduced HRQoL (all dimensions, but anxiety/depression) compared with NGJH. – Generally, the majority of OR for GJHS was nearly two times higher than the value for those with GJH alone. | GJH and specifically GJHS presented higher OR for upper body musculoskeletal symptoms, more severe symptoms, and decreased HRQoL. | |
| Di Stefano et al. (Italy) [33] | N/A | 27 adults with JHS | – JHS (BS ≥ 4 + Brighton criteria) – EDS-HT (Villefranche criteria) – DN4 questionnaire – fibromyalgia rapid screening tool – quantitative sensory testing – standard nerve conduction (assessing the non-nociceptive afferent fibres), and laser-evoked potentials (assessing nociceptive afferent fibres) | JHS vs EDS-HT vs NF | – Clinical examination and diagnostic tests showed no somatosensory nervous system damage. – Majority of patients suffered from widespread pain. The fibromyalgia rapid screening tool produced positive results, while quantitative sensory testing showed lowered cold and heat pain thresholds and an increased wind-up ratio. – Pain in JHS showed the mechanisms of fibromyalgia through central sensitisation compared to neuropathy. | In patients with JHS/EDS-HT, the persistent nociceptive input due to joint abnormalities probably triggered central sensitisation in the dorsal horn neurons and caused widespread pain. | |
| Johannessen et al. (Denmark) [27] | public | 52 adults with JHS/EDS-HT and 29 controls | – JHS (BS ≥ 4 + Brighton criteria)/EDS-HT based on the hospital record – Western Ontario Shoulder Instability Index (WOSI) – Numerical Rating Scale (NRS) – pain drawings – 36-item Short Form (SF-36) | JHS/EDS-HT vs NF | – HS/EDS-HT had lower shoulder function (WOSI total: 49.9 versus 83.3; p50.001), lower HRQoL on SF-36 Physical Component Scale (PCS: 28.1 versus 49.9; p50.001), and higher pain intensity (NRS: 6.4 versus 2.7; p = 0.001) than controls. – Neck and shoulder joints were rated as primary painful areas in both groups, with significantly higher frequency in JHS/EDS-HT (neck: 90% versus 27%; shoulder: 80% versus 37%). – Generalised pain was commonly reported by those with JHS/EDS-HT (96%), leading to reduced physical HRQoL. | – Adults with JHS/EDS-HT had impaired shoulder function, as well as frequent painful areas in the neck and shoulder joints, which needed to be targeted in the treatment strategy. – Adults with JHS/EDS-HT had reduced physical HRQoL compared to the general population. – Adults experiencing JHS/EDS-HT might present with both specific painful joints and generalised pain. | |
| Alsiri et al. (United Kingdom) [8] | public | 29 adults with JHS and 30 controls | – JHS (Brighton criteria), GJH (BS ≥ 4) – spatiotemporal parameters, joint kinematics, and joint kinetics (Qualisys motion capture system synchronised with a Kistler force platform) | JHS vs NF | – Statistically significant reductions in walking speed, stride length, and step length were found in the JHS group, while stance and double support durations were significantly increased (p < 0.01 ). – During the swing phase, the JHS group showed significantly less knee flexion (p < 0.01). – Reductions in hip extensor moment, as well as knee power generation and absorption, were identified in the JHS group (p < 0.01). Other gait parameters were not significantly altered. – Multiple gait impairments were found in those with JHS. | JHS group walked more slowly with a kinematic ‘stiffening’ pattern. | |
| Alsiri et al. (United Kingdom) [5] | public | 29 adults with JHS, and 30 controls | – JHS (Brighton and Villefranche) – Joint kinematics and kinetics (Qualisys motion capture system synchronised with a Kistler platform) tests were performed by jumping off from the floor to the level of ability and landing on both feet. | JHS vs NF | – Differences were not found in joint kinematics. – Sagittal hip and knee peak power generation were statistically lower in the JHS group during the compression phase (p ≥ 0.01), but not clinically relevant (SD < 0.5). – Clinically relevant reductions were found in the JHS group knee and ankle peak moments during the compression phase. Hip and knee peak power generation were observed during the push phase (SD ≥ 0.5), although these were not statistically significant (p ≥ 0.01 ). – JHS group achieved a similar jump height but with some biomechanical alterations. | JHS group achieved a similar jump height but with some biomechanical alterations. | |
| Jindal et al. (Canada) [43] | N/A | 106 Asian young adults | – GJH (BS ≥ 4 and Horan Joint Mobility Index) – Isometric strength of elbow and knee extensors was measured using an isokinetic dynamometer | GJH vs NF | – Male hypermobile subjects had significantly less strength than the non-hypermobile counterparts on the right (71.7 Nm, SD = 23.1, vs 97.6 Nm, SD = 47.4, p = 0.006 and left (74.8 Nm, SD = 24.3, vs 97.7 Nm, SD = 45.5, p = 0.007*) elbow extensors as well as right knee extensors (188.7 Nm, SD = 83.3, vs 228.3 Nm, SD = 106.7, p = 0.03*) – Females had no differences. | Males but not females with GJH had less isometric muscle strength in both elbow extensors and right knee extensors compared to non-hypermobile subjects. | |
| Ostuni et al. (USA) [35] | N/A | 24 adults (18–35 y.o.) | –JHS (BS ≥ 4) – visual analog pain scale (VAS) – McGill pain scale – resting arm angle – girth – pressure pain threshold – all domains of DOMS were measured over five days | JHS vs NF | – VAS reporting was significantly greater in the hypermobile group compared to the non-hypermobile, and there was a significant difference over time (after DOMS induced). | Individuals with JHS might experience greater DOMS and require more time to recover between treatment sessions. Therapists need to be aware of the tendency of JH patients to experience higher pain levels related to exercise, and treatment parameters should be adjusted appropriately. |
[i] BS – Beighton score, CL – Anterior Cruciate Ligament, DOMS – Delayed onset muscle soreness, EDSH – Ehler-Danhoss syndrome hypermobility, GJH – generalised joint hypermobility, HAGOS – Copenhagen Hip and Groin Outcome Score, HRQoL – Health-Related Quality of Life, JHS – joint hypermobility syndrome, LJH – local joint hypermobility, N/A – data not available, NF – normal flexibility, QoL – Quality of Life, VAS – Visual Analogue Scale, SF-36 – Physical Component Scale y.o. – years old
Table 4
Summary of the characteristics and main results of the case-control studies
| Authors (country) | Funding | Subject (population) | Measured variables | Comparison | Main results | Conclusion | |
|---|---|---|---|---|---|---|---|
| Trained adolescents | Frydendal et al. (Denmark) [25] | N/A | 19 GJH and 19 NF swimmers (13–17 y.o.) | – GJH (BS ≥ 5 and Rotès-Quérol test) – three prone lying, upper-extremity weight-bearing shoulder stabilometric tests – three prone lying, upper-extremity weight-bearing shoulder stabilometric tests – Surface electromyography (SEMG) was measured from the upper trapezius, lower trapezius, serratus anterior, infraspinatus, and pectoralis major muscles – Co-contraction Index (CCI). | GJH vs NF swimmers | – Adolescent competitive swimmers with GJH showed no shoulder sensorimotor control deficiencies or altered shoulder muscle activity pattern, except for decreased pectoralis major activity in the bilateral upper extremity that supported open eyes (p = 0.043). – Pectoralis major activity in swimmers with JH was altered. | – Swimmers with JH showed no shoulder sensorimotor control deficits. – Pectoralis major activity in swimmers with JH was altered. – Long-term effect of altered pectoralis major activity in JH should be investigated. |
| Liaghat et al. (United Kingdom) [16] | public | 19 GJH and 19 NF swimmers (13–17 y.o.) | – GJH (BS ≥ 5 and Rotès-Quérol test) – isokinetic and EMG measurements – Western Ontario Shoulder Instability Index (WOSI) questionnaire – Visual Analogue Scale (VAS) for current pain, as well as pain during the latest 24 hours and seven days – Maximum Voluntary Isometric Contraction (MVIC) – gagey hyperabduction, sulcus, and load-and-shift tests | GJH vs NF swimmers | – Swimmers with GJH produced significantly lower peak torque (0.53 vs. 0.60 Nm/kg; p = 0.047) and maximum work (0.62 vs. 0.71 J/kg; p = 0.031) than controls during medial rotation (60°/s). – Swimmers with GJH showed significantly larger isokinetic fatigue at 180°/s (0.321 J/repetition; p = 0.010), and tendencies to reduced levels of muscle activity in infraspinatus (20%, p = 0.066) and pectoralis major (34%, p = 0.092) at 60°/s during medial rotation. – Young competitive swimmers with GJH, despite no formal diagnosis, showed strength and fatigue deficits in medial rotation, potentially inherent with a greater risk of shoulder injury. | Young competitive swimmers with GJHS showed strength and fatigue deficits in medial rotation, potentially inherent with a greater risk of shoulder injury. | |
| Trained adults | Szuba et al. (Poland) [31] | N/A | 30 jazz dancers and 30 nondancers | – Benign JHS (BS ≥ 5 for females and BS ≥ 4 for males) – survey with questions related to physical activity, treatment of injuries, type of stabilising exercises, pain frequency and intensity (VAS Pain) | study group: jazz dancers control group: sedentary job workers | – BJHS was more common in the dancer group (27 subjects) than in non-dancers (9 subjects). – BJHS significantly correlated with the number of injuries in dancers (p = 0.02). – Number of stabilising exercises significantly correlated with less frequent pain (p = 0.04). | – BJHS was more common among the dancers than non-dancers and was related to pain occurrence. – Stabilising exercise alleviated pain. |
| Untrained adolescents | Nikolajsen et al. (Denmark) [6] | private | 16 females with GJH and 10 controls (14–15 y.o.) | – Asymptomatic GJH (BS ≥ 6 + at least one knee hyperextension) – Surface electromyography (sEMG) on quadriceps, hamstrings, and gastrocnemius muscles of the dominant leg during treadmill walking – Knee joint angles during treadmill walking were measured by electrogoniometer – Co-contraction index (CCI) | GJH vs NF | – Group differences were not found in demographics, muscle activation level, as well as CCI and CCI ratios during walking. – Subjects with GJH showed significantly decreased mean (153° vs. 156°; p = 0.03) and minimum (105° vs. 111°; p = 0.01) knee joint angles, during treadmill walking compared to controls. | Females with GJH had minor but statistically significant lower mean and minimum knee joint angles (increased knee joint flexion) during treadmill walking than a matched group without GJH. |
| Untrained adults | Bates et al. (United Kingdom) [20] | public | 23 adults with JHS, 23 GJH, and 22 NF | – JHS (Brighton criteria), GJH (BS ≥ 4) – electromyography outcomes (EMG) and kinematics for the lower limbs (Vicon motion capture system). – sudden forward perturbations test | JHS vs GJH vs NF | – There were no significant differences between groups in muscle onset latency. – At the first perturbation, the JHS group had significantly longer time-to-peak amplitude than the NF group in tibialis anterior, vastus medialis, rectus femoris, and vastus lateralis, as well as the GJH group in the gluteus medius. – JHS group showed significantly higher cumulative joint angle (CA) than the NF group in the hip and knee at the first, second, and sixth perturbation, as well as in the ankle at the second perturbation. Subjects with JHS had significantly higher CA than the GJH group at the hip and knee in the first and second perturbations. There were no significant differences in TTR. | – JHS group experienced greater instability. – Perturbation training might help for subjects with JHS. |
| To et al. (United Kingdom) [23] | public | 12 adults with JHS, and 12 controls | – JHS (BS ≥ 4 and Brighton criteria) – electrical stimulation of the musculocutaneous nerve to biceps brachii – transcranial magnetic stimulation over the motor cortex supplying biceps brachii | JHS vs NF | – JHS subjects experienced greater fatigue during the protocol compared to a control group and did not recover. – Central and peripheral fatigue did not occur in the control group. – However, the JHS group showed central fatigue. MEP amplitude increased in the JHS group during the fatiguing protocol (p < 0.01) before recovering. – Superimposed twitch amplitude increased in the JHS group during the fatiguing protocol and stayed elevated during the recovery phase (p < 0.04). – Time to peak (TTP) amplitude of the torque generated by the TMS was longer in the JHS group (p < 0.05). – RMS during MVCs decreased during the fatigue period and significance during the recovery phase (p < 0.01). | JHS subjects suffered central but not peripheral fatigue. |
Hypermobility measurements
The BS was used in the highest number of studies to determine JH, and the Brighton criteria were applied for JHS. A previous evaluation of JH was performed with the Horan Mobility Index, and the Rotès-Quérol test was carried out as an additional examination for shoulder, cervical, and lumbar spine mobility. A few among others used the Carter and Wilkinson criteria, while three determined EDS based on the Villefranche criteria.
Outcome measurements
The results showed that JH was commonly associated with pain, instability, muscle weakness, and delayed recovery. The majority of studies included in this review applied the visual analogue scale (VAS) as the pain scale parameter. Additionally, muscle stability and strength were evaluated using the Gait test and kinematic measurements, with Magnetic Resonance Imaging (MRI) and a standardised questionnaire.
Hypermobility and health problems
JH was known as a significant risk factor for many health problems affecting QoL, while trained [16, 26, 36] and untrained individuals with JH in this review had more fatigue compared to those experiencing normal flexibility (NF) [8, 22, 23, 27]. Furthermore, JH was associated with more musculoskeletal pain [35], less muscle strength [29, 32], and decreased proprioception [4, 6–8, 45]. Previous studies showed that JHS was a potential antecedent to pain hypersensitivity and central sensitisation syndromes, leading to disability [23, 26–28, 37]. The pain and risk of injury increased with training [15, 38, 45] because of muscle alteration and compensation in JH individuals to stabilise the knee or generate power when walking and jumping [4, 6–8, 45], as well as altered pectoralis major activation in swimmers with GJH [25]. Alteration was reported to cause higher knee compression, thereby increasing the future risk of osteoarthritis [4, 6–8, 45]. The proportional increase in the symptoms and the BS represented a positive correlation with joint laxity. Proper training could lead to adaptation in individuals with JH and prevent further injuries. Two studies recommended stabilising exercises [16, 31], and four suggested specific strengthening training for a minimum of 30 min per week to achieve less injury and pain [16, 22, 31, 32]. Self-guided low-resistance training showed no results on muscle strength improvement in untrained individuals with JH. Meanwhile, six studies suggested a designed training routine for improving muscle strength at the same rate between JH individuals and normal counterparts [20, 22, 23, 27, 34, 43], with Table 5 presenting the general results and clinical suggestions related to this observation.
Early assessment and appropriate training tend to provide benefits for individuals with JH. The main results, problems, and clinical suggestions proposed for both trained and untrained individuals with JH are presented in the subsequent sections. This research showed that JH among trained subjects could be acquired naturally or through training and from activity adaptation such as in dancers [15, 18, 24, 39]. Pectoralis major activity in swimmers with hypermobility was altered [25]. More frequent fatigue in subjects with GJH led to a reduced number of games played [16, 35, 36, 46], and GJH related to more pain and less muscle strength [29]. Training exposure significantly increased the risk of injury, while proper training could promote adaptation in individuals with JH, and prevent further injuries [19, 24, 30, 39, 41, 42, 43]. Stabilising and specific strengthening training (min. 30 min/week) helped to achieve less injury and pain [16, 31].
Factors found to influence JH among untrained subjects included age, gender, and activities such as dancing [28]. Others comprised socioeconomics roles, education of parents during gestation, and the possibility of children joining sports activities that could increase JH (e.g. dance, gymnastics, etc.) [45], while a higher BS cut-off was correlated with more symptoms [9, 45]. Muscle activation in individuals with GJH was altered or compensated, for example, to stabilise the knee or generate ankle power when walking or jumping. This explained why individuals with JHS were less stable, and the alteration could be the risk factor for osteoarthritis in the future [4–9]. Higher knee compression and decreased proprioception in GJH/JHS tended to increase the future risk of osteoarthritis [9, 35]. GJH was identified as a risk factor for musculoskeletal pain, and JHS was a potential antecedent to pain hypersensitivity and central sensitisation syndromes, which could lead to disability [23, 26–28, 33, 37]. The number of activities or training significantly increased the risk of injury and pain [15, 38, 45], while more frequent fatigue was observed in individuals with JHS [21, 23, 27, 35]. Self-guided low-resistance training did not improve muscle strength, while specialised training could enhance muscle strength at the same rate between individuals with JH and normal counterparts [5, 20, 22, 23, 29, 36, 45].
Clinical suggestions for individuals with JH include preparing different classifications of JH according to gender and profession [15, 18, 24, 39]. There is also a need to conduct early JHS assessment, provide family education [45], and investigate the long-term effect of altered muscle activity in JH [25]. The development of a new cut-off definition is essential for trained and untrained individuals with JH [9, 45], while rest periods and return-to-play time-scales should be respected. Less demanding alternative professions, which include teaching, can be considered over engaging as performers [16, 35, 36, 46]. Individualised functional training such as strengthening, stabilisation, perturbation-based training, and proprioception are needed to help improve muscle balance and strength. The use of braces and Kinesio tapes can be considered [19, 24, 30, 39, 41, 42, 44], specifically to prevent falling incidences, fear of falls, and low QoL [5, 20, 22, 23, 27, 34, 43]. Paediatric nurses should increase awareness to assess GJH in adolescents with chronic pain and recommend early functional training before the onset of pain [23, 26–28, 33, 37].
Discussion
Characteristics of survey contexts and methods
Among the studies included in this scoping review, eight were cohort (Table 2), 22 were cross-sectional (Table 3), and six were case-control (Table 4). The majority did not perform randomisation of subjects except for Luder et al. [34], and Nikolajsen et al. [6]. Only three conducted randomisation on data or subject recruitment [9, 27, 44], and a few used less than 20 subjects per group, which could be improved [6, 9].
Only studies on adolescents and adults were included in this scoping review because JH-related problems and injury risk did not significantly affect children and were found to increase with age. The majority of studies extracted were conducted in Europe, and only one in Asia, which has a higher prevalence of JH [47]. Therefore, the awareness of JH as a risk factor for health disturbance was presumed to be lower in Asia. The adolescent and adult populations reviewed had similar results, where hypermobile adolescents without proper training developed more pain and fatigue, as well as reduced physical fitness levels. This signified the importance of detecting the condition early to prevent further injuries or even disability [24, 48]. The amount of training in athletes and professionals, including dancers, could increase JH but could also induce the adaptation of muscle activation naturally. Morris et al. [45] uniquely associated the severity of JH with deficient maternal education in lower socioeconomic strata and lifestyle preferences in the higher socioeconomic status; hence, public education related to JH might be beneficial.
Hypermobility assessment
The BS and Brighton criteria were the predominantly used parameters and simplest methods to determine JH and JHS. Validity studies on the BS showed a sensitivity of 0.8% and a specificity of 99.3% p < 0.001). To lower the high false-positive rate (~60%) using a cut-off of ≥ 4, further JH tests were conducted [49]. Previous studies found that the cut-offs of the BS and Brighton criteria should be reviewed and updated [18, 24, 28, 39, 42]. Factors contributing to JH included age, gender, genetics, and training; hence, different classifications of JH should be prepared according to gender and profession, such as for dancers requiring a more restricted BS cutoff (≥ 6) [50].
The BS evaluates only a few selections of joints, focusing on the upper body while excluding frequent injuries in the lower limbs of dancers [51]. Active forward flexion of the trunk in the BS could be ambiguous due to the potential reflection in hamstring length than in spinal mobility [45]. Other methods should be integrated while assessing different professions to determine the contribution of the lumbar spine, such as the Upper Limb Hypermobility Assessment Tool (ULHAT) and Lower Limb Assessment Score for dancers [52], and the Schobers modified test [18].
GJH often showed no symptoms, and most affected individuals were unaware of the presence, but incorrect training could prompt GJH to contribute instability and microtrauma to the affected joint structures [39]. The need to define a new classification for NF, asymptomatic GJH, and JHS was identified due to genetic factors, such as EDS requiring different treatment strategies, while genetic markers could be developed for JH and the degree of severity [40].
The assessment of hypermobility should be included as part of medical screening in schools, sports clubs, and the military to avoid future chronic injuries and maximise the potency of JH individuals in the field. This can provide an awareness of a more important health problem, such as a hereditary disorder of connective tissue. Therefore, professional education needs to be recommended, particularly for primary practitioners regarding the complex diagnosis of JH [40].
Hypermobility and health problems
Children with GJH usually experience pain when transitioning into puberty, which may be due to hormonal changes as well as an imbalance in the growth of bone and soft tissues [24]. Therefore, paediatric nurses should be equipped with JH assessment knowledge and be aware of chronic pain symptoms in children and adolescents. Children diagnosed with JH commonly showed better performance in some sports. There is a need to promote public education efforts aimed at ensuring optimal performance and protecting children from overtraining, which can cause ligament injuries and dislocations (with JH condition) [8, 45].
Hypermobility can be asymptomatic (GJH) and symptomatic (JHS); specifically, adolescents with asymptomatic GJH showed no significant differences in muscle strength or pain compared to their non-JH peers [28]. Meanwhile, adults with JH may experience greater pain and require an extended time to recover [35]. Several cohort studies should be performed to observe the potential development of this condition into a symptomatic state at puberty. In JH individuals, the activation of muscle is often altered or compensated [4, 6–8, 45] to address the joint instability and avoid pain. Bates et al. [20] previously reported that the alteration was adopted individually, showing the tendency of subjects to address the stability challenge through different methods. This alteration can increase the risk of osteoarthritis in the long term [4, 6–8, 45], signifying the need to determine whether asymptomatic JH adolescents will develop the risk over time.
Individuals with JHS (but not GJH) in the majority of the reviewed studies experienced lower QoL. The results showed that joint instability reduced neuromuscular control, and increased ROM, causing frequent discomfort in individuals with JHS. These individuals tended to avoid sports or recreational activities due to a fear of movement from subluxation risk, dislocation, pain, injury, or potentially trauma after experiencing injuries. However, the fear of movement could lead to physical inactivity and limit daily life functions [27]. Certain studies reported no difference in pain or rates of injuries, particularly among trained subjects [24, 41, 44].
Fatigue is another problem in individuals with JHS that initiates lower QoL and psychological comorbidities. Individuals with JHS increase or decrease specific muscular activity (compensatory mechanism) to stabilise joints. The compensatory mechanism becomes more difficult in a high-intensity task [8], leading to chronic pain [8]. The ability to stiffen joints during high-intensity tasks reduces the pain and recurrent injury but may lead to fatigue [8].
Stefano et al. [33] suggested that the pain in hypermobility was underpinned by central sensitisation compared to neuropathic pain reflection. Therefore, trained subjects such as athletes tend to suffer from less pain and injuries compared to non-trained counterparts. This is attributed to their high training volumes, which impact mental health and often reflect an altered perception of pain, fatigue, QoL [23, 24, 46], and pain tolerance [43].
Clinical suggestion for hypermobility
An early JH assessment as well as the provision of education for family and primary healthcare workers is beneficial to managing the activities of affected individuals. This assessment assists in preventing chronic injuries and maximises their potential, specifically for those participating in dancing or gymnastics [8, 45].
Individuals with JH in the majority of studies experience more fatigue compared to their non-JH peers, due to their reduced muscle strength [29] and decreased proprioception [4, 6–8, 45]. Therefore, rest periods and adequate nutrition, specifically protein intake, need to be respected since fatigue can increase the risk of incorrect movements, overuse, and falls, which all lead to injury [50]. Less demanding profession alternatives should be considered, such as engaging in teaching over being a performer [16, 29, 36].
There were no significant differences in injury rates observed in the majority of studies between trained individuals with JH and their non-JH peers. The amount of training contributed more significantly to injuries than the JH [15, 38, 45], showing that trained individuals have developed muscle strength to the same degree as their non-JH counterparts. To and Alexander [22] reported that individuals with JHS possessed the same rate of muscle strengthening as others but with different baselines. Therefore, the exercises should be adjusted to a minimum of three times per week and started at a level appropriate to their functional ability. The resistance needs to be increased gradually every six weeks because there will be no improvement afterward due to muscle adaptation [34].
JH was observed in this study to vary between subjects depending on gender, genetics, early age activity, profession, and awareness, which could lead to different symptoms, pain tolerance, and joint adaptation. According to the different degrees and symptoms, personalised training should include proprioceptive, perturbation, and postural balance exercises to correct alignment and the accurate range desired for each joint, specifically the shoulder, elbow, hip, and knee [7, 20, 31, 53]. Enhanced proprioception serves as a preventive measure against hyperextension movements. Achieving this requires strength training designed to maintain optimal performance, which is particularly relevant for dancers, while simultaneously mitigating the risk of overloading [53].
Future perspective
Biological adjuvants can be used in addition to physical training and early assessment to enhance muscle strength in hypermobility for preventing or repairing injuries in muscles and joints. Further studies or systematic reviews including the benefit of using biological adjuvants such as mesenchymal ‘stromal’ cells (MSCs) or MSC-secretome may show interesting results to complement current knowledge.
Research limitations
Limitations observed in this study included the failure to conduct a methodological quality evaluation. Additionally, the difference between JH subjects based on genetics or training was not analysed because both had the same risk of injury and would obtain similar benefits from proper strategies. Only English literature was included in this study despite the tendency of publications in other languages to deliver useful data. A further exploration through meta-analysis, featuring a greater number of databases with clearer inclusion and exclusion criteria, could facilitate a better assessment and management of individuals with JH.
Conclusions
This study identified the tendency for society to ignore JH, even in professional healthcare. Certain individuals thought being hypermobile was an advantage, specifically when requiring JH in careers such as gymnastics or dancing. However, symptomatic and asymptomatic JH showed the risk of chronic injury, which could decrease activity and QoL in the future. The injury risk factors in JH and the strategies to prevent further injuries among those affected were comprehensively reviewed. In general, the BS was found to be predominantly used in determining JH, and the Brighton criteria were applied to JHS, as described by Engelbert and Rombaut [1]. JH acquired naturally and through training [10] was commonly associated with pain, instability, and muscle weakness, as well as fatigue, and decreased QoL. Therefore, early assessment, public education, and individualised training would be required to prevent chronic injuries.
Furthermore, the tendency to ignore JH was observed, especially in the Asian population, which feature a high prevalence. The majority of individuals with JH suffer from chronic pain, muscle instability, weakness, and fatigue, leading to QoL decline. Adequate nutrition intake, along with specific and individualised training at least three times per week, should be designed based on the degree and symptoms of hypermobility. These would include proprioceptive, perturbation, adequate strength, and postural balance exercises to correct the alignment and accurate range desired for each joint, specifically the shoulder, elbow, hip, and knee. Early comprehensive assessment and proper management were recommended to protect individuals with JH from future chronic injury and reduce the public health burden of pain management.