Introduction
The suboccipital muscles (sOMs) primarily function to provide dynamic stability to the upper cervical spine. They perform small pendulum-like movements in the craniocervical junction, ensuring a neutral head position and offering proprioceptive feedback to the central nervous system [1]. The abundance of proprioceptors within the sOMs underscores their role in proprioception [2].
The highly delicate proprioceptive system of the cervical spine, which plays a crucial role in body posture and balance control [3], communicates the position of the head relative to the trunk, coordinates with the vestibular and visual systems, and is vital for the maintenance of body posture and balance [4]. Overloading the sOMs often presents as reflex changes, such as the development of myofascial trigger points (TrPs). These TrPs are characterised as hyperirritable spots within a muscle, manifesting as tender nodules palpable within taut bands [5, 6]. Upon palpation, these points are painful and may radiate pain unilaterally deep into the occipital region, as well as into the temporal area, eyes (ocular mask), and forehead. While patients typically localise the pain to the base of the skull, it is not directly associated with headache pain from the splenius cervicis muscle but rather with tension-type headaches [7, 8]. Disruption of cervical proprioception is a common issue in patients with neck pain, leading to disturbances in cervical sensorimotor control [2]. These disturbances can result in long-term changes in muscle tissue, exacerbate pain through peripheral and central nervous system mechanisms, sensitise the system, and contribute to dysfunctional movement patterns [1]. Moreover, muscle pain affects motor control strategies through central mechanisms [9, 10]. Research has shown that structural and functional alterations in the sOMs can influence muscle spindle firing or sensitivity, affect ing afference and leading to the aforementioned proprioceptive changes. As a result, flawed proprioception distorts the direct linear interaction between cervical proprioception and vestibular information, leading to an imprecise, subjective body orientation and spatial psychological representation (soma- tognosia). This can manifest as dizziness or a subjective sense of instability [11].
Examination of trigger points in the suboccipital muscles
Individuals with TrPs in the sOMs often experience headaches and exhibit a forward head posture, which is a common abnormality observed in clinical conditions affecting the cervical spine. The extension of the upper cervical spine in this posture results in the compression of cranio-cervical structures, especially the suboccipital and posterior cervical muscles. Visual assessment is a common method for evaluating an individual’s body posture, with numerous studies indicating that manual evaluation of upper cervical dysfunction can assist in the precise diagnosis of patients experiencing cervical headache pain [12-14]. Proper manual assessment is crucial for distinguishing between TrPs in the sOMs and dysfunction of the craniocervical joint. it is important to note that the area just below the skull, where the sOMs are located, is highly sensitive to palpation, and therapists should be mindful of the pressure applied. Since the sOMs muscles are overlapped by the upper trapezius and other posterior neck muscles, they cannot be directly palpated. However, applying pressure to the anatomical projection of the sOMs can elicit pain specific to these muscles, distinct from the pain experienced in the splenius capitis or upper trapezius muscles. Additionally, palpation of each sOM may evoke slightly different pain patterns in some patients. Fernandez de las Penas et al. [15] developed a protocol for diagnosing TrPs in the soMs, which includes assessing sensitivity in the suboccipital area, pain elicited by sustained pressure, and increased pain radiation during muscle contraction with upper cervical spine extension.
Assessment of sensorimotor control
According to the existing evidence, it is advisable for individuals with neck pain to undergo evaluation and treatment for impairment in cervical proprioception and disorders in sensorimotor control [16]. There are eight tests available to evaluate neck sensorimotor control in patients with chronic neck pain, including the Joint Position Error (JPE) test, posturography assessment, Subjective Visual Vertical test, Head Tilt Response test, Fly test, Smooth Pursuit Neck Torsion test, Head Stiffness test, and Rod-and-Frame test [3]. These tests may include assessing various subsystems involved in sensorimotor control, such as the oculomotor and vestibular systems, in addition to measuring cervical sensorimotor control [17].
Posturography measurement is a time-efficient technique that has proven useful in detecting significant changes in body sway during challenging situations. The implementation of force spectrum analysis in posturography testing can be a valuable tool for improving the evaluation of cervical spine function and monitoring rehabilitation treatments [18]. Head movements are also utilised in posturography measurements, which, according to several authors, significantly increase the movement of the centre of pressure (CoP) of the reacting force on the support surface [19, 20].
Treatment of trigger points in suboccipital muscles, neck pain, and headache
Various treatment approaches are used for cervicogenic headaches associated with TrPs in the soMs. These approaches include electrotherapy, kinesiotherapy, and manual techniques [21]. Manual techniques employed for trigger point inactivation include ischaemic compression, combined trigger point compression with active muscle contraction, spray and stretch, post-isometric relaxation, and neuromuscular approaches [22]. Evaluating the most effective manual approaches poses a challenge since most therapists adopt a multimodal approach [23]. Corrective measures involve postural correction, ergonomic assessment, strengthening exercises, and self-stretching. Karegeannes et al. [16] recommend maintaining neck warmth, adjusting head position during daily and work activities, and ensuring proper overall body posture. They suggest stretching short and long neck extensors with manual patient assistance and placing a hand under the occipital bone, although manual therapy is not specifically mentioned. Though manual therapy targeting TrPs in the soMs and related headache pain might yield positive outcomes in terms of pain intensity and frequency, additional research is needed to enhance the evidence regarding the impact of manual therapy on individuals suffering from tension-type headaches [24]. Specifically, the myofascial release technique (MFR) focuses on releasing shortened muscles and tension [25]. MFR utilises gentle pressure and stretching through direct and indirect approaches with the intention of reducing pain, optimising muscle length, and releasing fascial restrictions caused by injury, stress, or repeated static loading [26]. According to Ramezani et al. [25], the application of MFR and regular exercises leads to a rapid and early reduction in pain intensity, frequency, and pressure pain threshold in patients with cervicogenic headaches. As mentioned earlier, treatment of proprioceptive disorders and sensory-motor control disturbances should be considered in patients with neck pain as it can have a positive impact on improving proprioception in the cervical spine area, chronic neck pain, cervical spine and balance function, and cervicocranial joint function [27]. Proprioception in the cervical spine area may improve through pain modulation or reduction, although research has yet to confirm this [3]. However, it is important to reduce muscle tension in the neck caused by pain to improve postural functions, which may lead to the normalisation of proprioceptive signals from neck muscles and a reduction in sensory-motor mismatch. Specific local treatment for neck pain relief that improves sensory-motor function is not discussed [3].
objective of the study
Our study investigated the immediate impact of MFR on postural stability in patients with TrPs in the soMs. While the effect of MFR on neck pain is well-known, the influence of MFR on the current state of proprioception and postural stability remains uncertain, and this was the primary focus of our study.
Subjects and methods
Characteristics of the study sample
The study included 12 patients diagnosed with TrPs in the soMs (eight females and four males aged 37 ± 9.5). Participants were selected from patients seeking rehabilitative treatment for headaches associated with suboccipital pain and identified TrPs in these muscles. We used power analysis to determine the sample size, ensuring a sufficient number of participants for statistical validity. To ensure that all patients met the inclusion criteria for the study, they underwent a cervical spine examination conducted by a single experienced physiotherapist with over 15 years of practice. This examination included a patient interview, detailed medical history taking, a review of the patient’s entire medical documentation and findings, if available, and a palpation examination of the soMs.
Based on the CARE (case report) guidelines, we structured and wrote this case report to ensure a systematic and transparent description of the clinical case. The inclusion criteria for patient enrolment were adults within a specified age range, a forward head posture, TrPs in the soMs with referred pain elicited by sustained manual pressure, a sensation of instability while walking but not true vertigo, and headaches occurring at least once a week in the last month. These criteria ensured that the study focused on the target population with relevant clinical characteristics. Exclusion criteria for the experimental group of patients were the manifestation of autonomic system symptoms, vertigo, or visual disturbances, severe distinct neck pain attributed to a herniated disc, spinal canal stenosis, or cervical spondylosis, any condition that might contraindicate the use of the MFR technique in the upper cervical region, and undergoing physiotherapy for neck and headache pain within the past week.
The control group consisted of 12 healthy individuals (7 females and 5 males aged 25 ± 3) without any headaches, neck pain, musculoskeletal disorders of the cervical spine, or TrPs in the soMs upon palpation.
Course of measurement
This experimental study focused on determining the immediate effect of myofascial techniques on postural stability in patients with reflex changes in the upper cervical region. During the initial clinical examination, postural stability was assessed using a stabilometric platform (Freestep Software; Sensor Medica, Rome, Italy). The platform’s overall surface area measures 635 mm x 700 mm, while the active sensor surface spans 500 mm x 600 mm. Real-time sampling occurs at a frequency range of 300-350 Hz. Subsequently, the patients received MFR in the upper cervical region (Figure 1), as described in detail in the study by Ramezani et al. [25]. The total treatment duration was up to 10 min, and immediately after the treatment, all patients, as well as participants in the control group, underwent repeated posturographic examination. The examination was then repeated for all participants after an hour of rest.

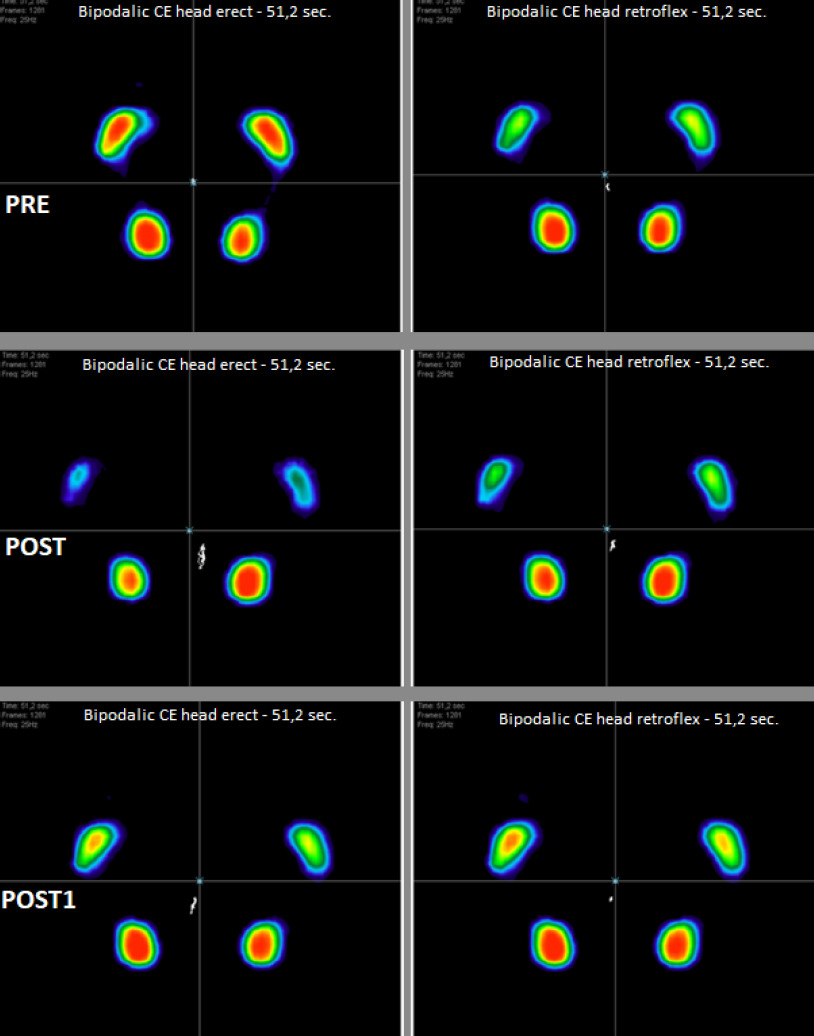
During the stabilometric assessment, body oscillations were evaluated by placing the subject on a force platform (Sensor Medica, Rome, Italy) in an upright position with arms at the sides, heels approximately 4 cm apart, and the forefoot rotated outward at an angle of 30°. This assessment was performed using the cervical test (Freestep software; Sensor Medica, Rome, Italy), which involves (1) standing with an upright head posture and eyes closed for 51.2 s, in accordance with the Romberg test, and (2) standing with head retroflexion and eyes closed for 51.2 s (Figure 2). The head retroflexion posture is explained by several authors as causing deaffer- entation of proprioceptors in the cranial region, which is crucial for maintaining postural stability [28]. Posturographic recordings with the patient’s head in retroflexion have been proposed as a reliable and sensitive test for diagnosing stability related to cervical dysfunction and as a diagnostic “fine- tuning” of stabilometry [29].

Measured parameters and data processing
To evaluate postural stability, we used parameters that characterise the movement of the Center of Pressure (CoP) in a standing position (Figure 3). The displacement of CoP was analysed by assessing (1) CoP trajectory length, (2) CoP ellipse area, (3) mean CoP velocity, (4) mean CoP displacement in the anteroposterior direction, (5) mean CoP displacement in the mediolateral direction, (6) standard deviation of CoP movement in the mediolateral direction, and (7) standard deviation of CoP movement in the anteroposterior direction.
The data collected underwent processing using Statis- tica 13.0 software (TIBCO Software Inc., CA, USA). Given the limited number of subjects in the experimental group, we employed the non-parametric Wilcoxon rank-sum test to evaluate the significance of differences in the measured values. Differences were deemed significant at a = 0.05.
Results
The immediate effect of manual treatment on reflex changes in the sOMs on postural stability was demonstrated in almost all assessed stabilometric parameters (Table 1). Under the condition of standing with an upright head posture and closed eyes, there was a statistically significant rise in postural instability following the therapeutic intervention, with significance noted at p < 0.05. The length of the CoP trajectory was 450 ± 127 before MFR treatment (pre) and 607 ± 168 after MFR treatment (post) (p = 0.02). The area of the CoP ellipse was 95 ± 112 before treatment (pre) and 218 ± 158 after treatment (post) (p = 0.03). The mean speed of CoP movement was 10 ± 2 before treatment (pre) and 11 ± 4 after treatment (post) (p = 0.03). The mean value of CoP movement in the anteroposterior direction was -14 ± 10 before treatment (pre) and -26 ± 9 after treatment (post) (p = 0.04). The standard deviation of CoP movement in the anteroposterior direction was 1.8 ± 0.7 before treatment (pre) and 2.3 ± 1 after treatment (post) (p = 0.01). In the lateral direction, it was 1.8 ± 0.8 before treatment (pre) and 4.4 ± 2 after treatment (post) (p = 0.04). After one hour of rest (post1), the assessed stabilometric parameters did not significantly differ from the pre-values in the standing position with an upright head posture.
0.02].
Table 1
Comparison of stabilometric in the experimental group
[i] Pre - before treatment, Post - after treatment, Postl - one hour after treatment, CoP X mean - mean value of CoP movement in the anteroposterior direction, CoP Y mean - mean value of CoP movement in the mediolateral direction, CoP Y SD - standard deviation of CoP movement in the mediolateral direction, CoP X SD - standard deviation of CoP movement in the anteroposterior direction * statistically significant value
In the control group, significant changes were only observed in the length of the CoP trajectory in an upright stance between pre (511 ± 210) and post (602 ± 162) measurements (p = 0.03) (Table 2). In the head-tilted stance, significant changes were also observed in the length of the CoP trajectory after treatment, which persisted even after one hour of rest [pre (450 ± 190) vs post (474 ± 217)], p = 0.02; post1 = 486 ± 168, p = 0.04). Significant changes were also noted in the mean velocity of CoP shortly after treatment [pre (10 ± 3) vs post (10 ± 2), p =
Table 2
Comparison of stabilometric parameters in the control group
[i] Pre - before treatment, Post - after treatment, Postl - one hour after treatment, CoP X mean - mean value of CoP movement in the anteroposterior direction, CoP Y mean - mean value of CoP movement in the mediolateral direction, CoP Y SD - standard deviation of CoP movement in the mediolateral direction, CoP X SD - standard deviation of CoP movement in the anteroposterior direction * statistically significant value
Discussion
The objective of this study was to investigate whether the MFR technique would have an effect on stabilometric parameters in patients with TrPs in the soMs. Surprisingly, the results indicated a worsening of certain stabilometric parameters immediately after the MFR treatment.
While many studies have focused on the effects of myofascial techniques and other manual therapy approaches on TrPs in the soMs, they mostly describe subjective improvements such as pain relief or increased range of motion in the cervical joints [7, 18, 23]. However, the impact on postural stability has not been explored. it can be assumed that TrPs in the soMs significantly influence postural stability because the upper part of the cervical spine plays a crucial role as a communication centre for mediated and coordinated reflexes that help maintain body position. Therefore, any intervention in these muscles can elicit an unexpected reaction from the postural system.
Although these findings contradict the results of several studies examining the impact of manual therapy on postural control, we did not find any studies investigating postural stability immediately after soM therapy, nor any studies examining the effects of any manual technique on soMs in relation to postural stability. A similar study by Fisher et al. [30] examined the immediate impact of cervical spine manipulation on postural stability, but their study failed to demonstrate any influence on CoP parameters. Additionally, Amato et al. [12] demonstrated improvements in some stabilometric indicators after self-treatment with the MFR technique in patients with migraines following 10 days of therapy. Similarly, Reid et al. [31] reported improved postural stability in a head- tilted standing position in patients with dizziness and neck pain after mobilisation techniques in the cervical area, but the improvements persisted after several weeks of observation.
Some authors have examined the effects of manipulative techniques on the cervical spine in asymptomatic individuals and found improved postural control after a single manipulation [14, 32]. As for the treatment specifically involving manual therapy in the cervical spine and its impact on postural stability, several explanations have been presented in the literature to account for the results of our study. However, all of these studies investigated MFR on postural stability after an extended period following the intervention (days to weeks).
The most significant factor associated with CoP deviations in patients with symptoms indicating cervical spine disorders is pain. Schabrun et al. [33] illustrated alterations in the somatosensory cortex during and post-pain, whereas modifications in the motor cortex occurred solely after pain cessation, exerting a more pronounced effect on CoP deviation. All patients in our study reported neck pain, which may have influenced the results. Moreover, patients with TrPs in the soMs also reported head pain when placing their heads on a pillow, which can be explained by the effect of the weight of the occipital bone on TrPs in the suboccipital region [6].
Abnormal cortical processing of proprioceptive information during neck pain and its impact on postural stability has been described by several authors [34, 35] and supported by theories suggesting that muscle spindles increase their resting excitability by up to 200 % after muscle stretching compared to pre-stretch conditions [36]. Although the MFR technique does not directly stretch the muscles, it still leads to increased muscle spindle response and delayed muscle relaxation after muscle contraction [37]. despite these theories, Peng et al. [3] point out in their narrative review on impaired proprioception in neck pain that high-quality research in this area is still lacking. Passive head movements, which are part of manual therapy, as well as changes in position from lying to standing, may also impact increased CoP deviations in patients with long-standing cervical spine difficulties [30, 33]. Burstein et al. [7] also mention an important factor related to changes in CoP deviations, namely that muscle relaxation in the cervical spine area through MFR causes a sudden vas- odilatory effect. Another theory worth mentioning is “sensory weighting”, which suggests that the postural and central nervous systems can reorganise the hierarchy of sensory information and prioritise other systems when the quality of sensory information is compromised, such as the vestibular system or proprioception from the lower limbs. [38, 39]. Hypothetically, such sensory weighting could have occurred in the patients in this study, and after intervention with TrPs in the soM, it could have led to a new reorganisation of sensory information, potentially resulting in larger CoP deviations.
Limitations
The primary constraint in our study was the limited sample size, which was a result of excluding discrete subjects. Assessing stability parameters at earlier time intervals following MFR treatment would provide a more precise understanding of when stability adjustments occur and give more accurate insights into the timing of stability adjustments after MFR treatment.
Conclusions
In this study on the influence of the MFR technique on postural stability immediately after its application, we observed significant differences in posturographic parameters, indicating increased instability in patients compared to their pre-therapy state. The patients received myofascial treatment for TrPs in the soMs. However, after an hour of rest, the patients’ postural parameters were adjusted and normalised. The myofascial technique also had an impact on healthy individuals in the control group, particularly on the trajectory of the CoP. overall, the influence of MFR on postural stability was much smaller in healthy individuals without TrPs in the suboccipital region. These results support the theory that therapeutic intervention in the upper cervical spine affects proprioception from that area and postural stability.
For safety reasons, we recommend that patients remain in a stable position that does not require significant postural stability after therapy. This is particularly important for patients scheduled to undergo additional kinesiotherapy after manual therapy, as it could affect safety and the quality of exercise. These findings could contribute to improving the safety and quality of rehabilitation treatment for patients.