Introduction
The hamstrings do not independently control the movements of a single joint; rather, they contribute to dynamic movements by concurrently manipulating multiple joints, such as the hip and knee [1,2]. For example, during walking and running, hip and knee flexion occur simultaneously during the swing phase [3]. From a single joint perspective, hip flexion is defined as an eccentric contraction of the hamstrings, while knee flexion is defined as a concentric contraction of the hamstrings [4]. However, because the movement occurs at both joints simultaneously, the increased length of the hamstrings due to hip flexion is partially offset by the knee flexion. This mechanism of maintaining optimal length–tension relationships helps produce force and torque stably throughout the range of dynamic movements [5]. In addition to hip and knee flexibility, ankle flexibility plays an important role in lower-extremity function, especially during sports and daily activities [6]. In the presence of hamstring tightness, knee extension may be limited to the terminal swing, which can decrease gait speed [7]. Similarly, limited ankle dorsiflexion can affect lower limb biomechanics, increasing the risk of injury [8].
Stretching, which can prevent deficits caused by muscle tightness in the lower extremity, is widely performed in clinical practice [9, 10]. Just as professional athletes routinely stretch before exercise despite a lack of muscle shortening, ordinary people routinely stretch before exercise regardless of tightness status. However, most stretching studies targeting the general population have focused on individuals with hamstring tightness [11–13]. Thus, studies of subjects with normal flexibility are lacking, resulting in an imbalance in the verification of the effects of stretching on flexibility and leading to gaps in knowledge. In a previous study that examined individuals with normal flexibility, stretching induced a significant increase in flexibility [14]. However, the acute effects of stretching on flexibility were not confirmed, while those of a warm-up (WU) before stretching were not investigated.
In the field, a WU is usually performed before stretching to lightly relax the body [15]. In experimental settings, an active or passive WU is usually performed before flexibility measurements to reduce errors that can occur from a cold start. According to Atha et al. [16], range of motion gradually increased during 10 successive hip flexion tests. Therefore, an active WU should precede flexibility measurements [17–19]. However, the quantitative resistance that occurs during tissue elongation may vary depending on the flexibility of the hamstrings and other associated structures, including the ankle joint, which may lead to different outcomes in WU effectiveness between individuals with varying levels of tightness.
This study aimed to examine the difference in the acute effect of WU and stretching on lower-extremity flexibility, specifically in the hip, knee, and ankle, between individuals with hamstring tightness (HT group) and those without it (NoHT group).
Subjects and methods
Subjects
The sample size was calculated using G*Power 3.1.9.7 (Heinrich-Heine Universität Düsseldorf, Düsseldorf, Germany), with an effect size of 0.25, an α error probability of 0.05, and a power of 0.95 [20]. The statistical test used was ‘ANOVA: repeated measures, within factors’, which accounts for differences across multiple levels or conditions. Participants were voluntarily recruited through an online Google form. Participants with a history of hip or knee surgery or those who had experienced pain in the past 6 months were excluded. Hamstring tightness was assessed using the AKE test by a licensed physical therapist. Participants with an AKE > 20° after WU were classified into the HT group, while those with an AKE ≤ 20° were classified into the NoHT group [21,22].
Procedures
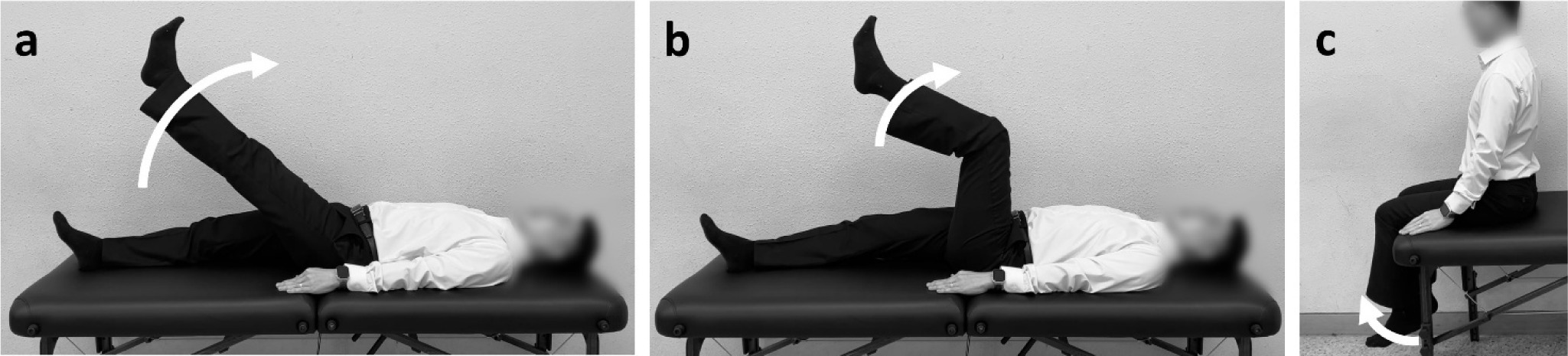
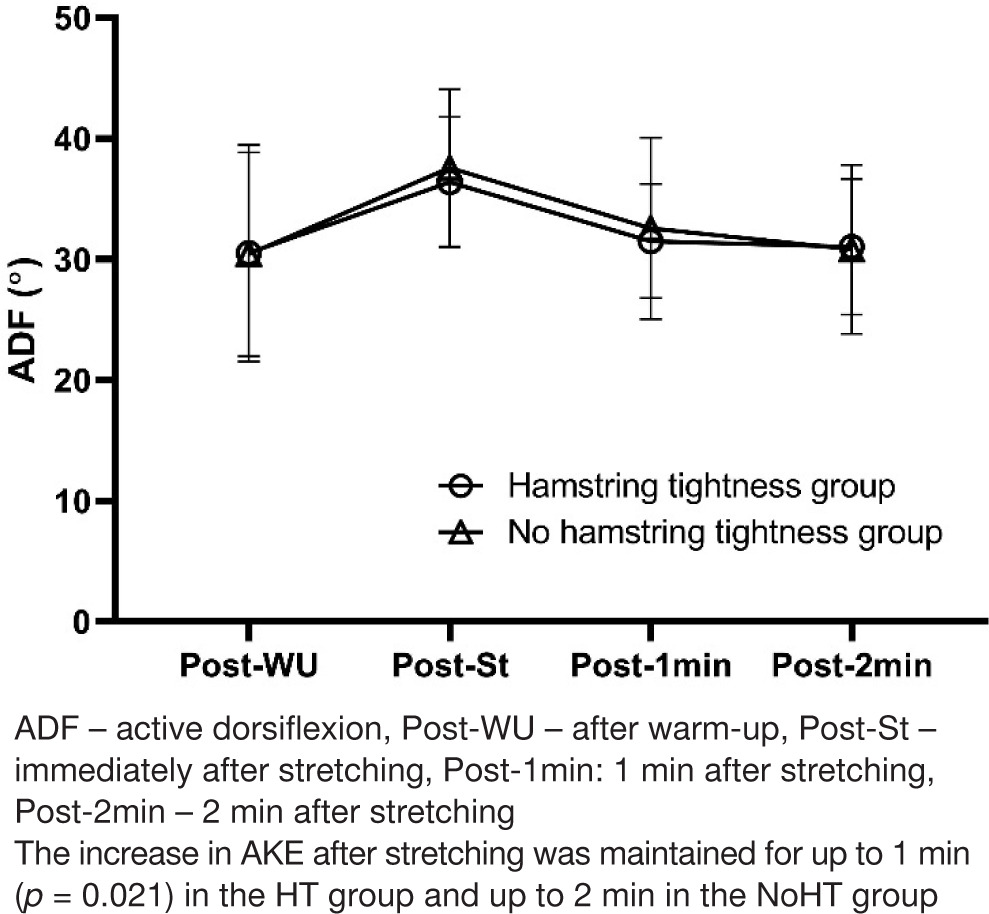
Flexibility was obtained by performing the AKE test twice, and the average value was recorded as the pre-WU. An additional six AKE repetitions were performed as the WU. To examine the effect of WU, ASLR (Figure 1a), AKE (Figure 1 b), and ADF (Figure 1c) were performed twice, and the average value was recorded post-WU. Flexibility measured after stretching was recorded as post-St (average of two measurements), flexibility measured 1 min after stretching was recorded as post-1 min (average of two measurements), while flexibility measured 2 min after stretching was recorded as post-2 min (average of two measurements). The joint range of motion (ROM) was measured using a digital inclinometer (Plaincode Software Solutions, Gunzenhausen, Germany), which was installed as an application on an iPhone 14 [22–24].
Each lower-extremity flexibility test was performed on the right leg. Following the examiner’s instructions, the subject slowly performed AKE [19]. During knee extension, a metal frame was placed under the lower leg to maintain 90° flexion of the hip and knee. The subject performed knee extension until discomfort or pain was felt; if myoclonus occurred, the knee was slightly flexed [25, 26]. SLR was also measured with the participant in the supine position [27]. The subject slowly performed hip extension until discomfort or pain was felt and held it for a moment at the endpoint of the ROM measurement. To prevent substitution, the participants were instructed not to push the treatment table with either hand. ADF was measured with the participant in a sitting position [22]. While maintaining 90° of hip and knee flexion, the subject slowly performed ankle dorsiflexion. The upper body was not allowed to lean back during the ankle dorsiflexion. ROM was measured by holding that position for a while at the endpoint.
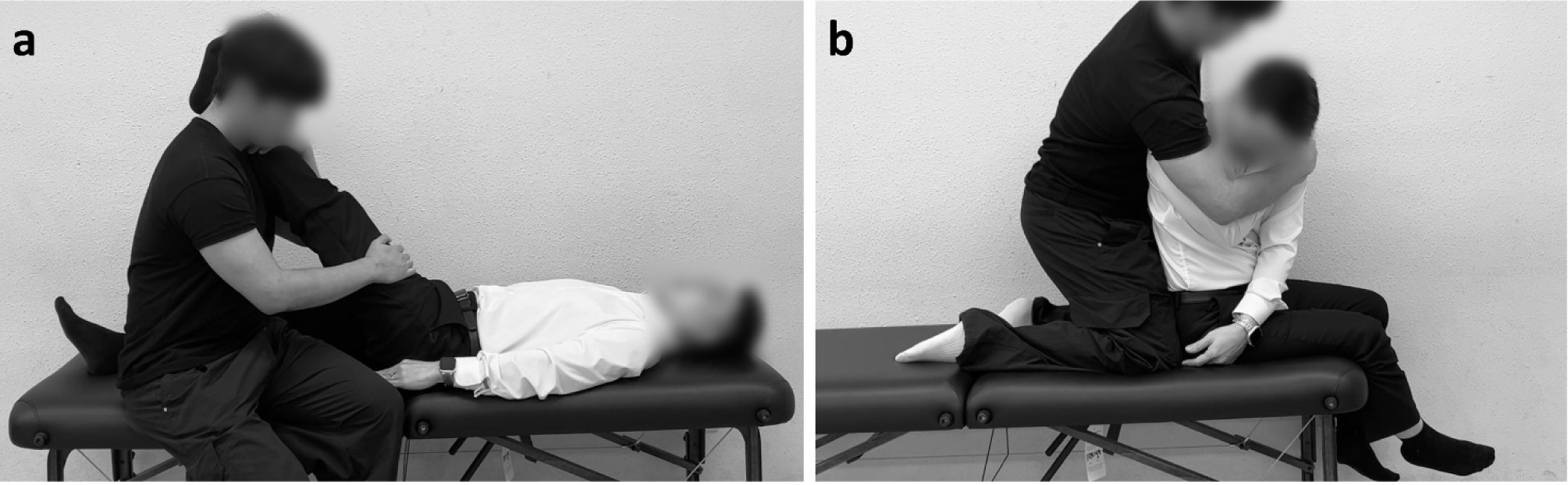
Stretching was applied sequentially to the lower and posterior trunks. The proprioceptive neuromuscular facilitation stretching technique was used on the lower extremities (Figure 2a) [19]. The subjects slowly performed hip flexion while in the supine position with the knee fully extended. At the endpoint, hip flexion was performed, and the examiner applied resistance in the opposite direction to induce maximal voluntary isometric contractions (MVIC). The MVIC was performed for five trials of 6 s/trial. The static stretching technique was used to stretch the posterior trunk (Figure 2b) [28, 29]. Each subject sat in a neutral pelvic position, placed the right hand on the left shoulder, and rotated the trunk with flexion while exhaling slowly. At the endpoint, the examiner applied additional tensile stress to stretch the tissue. Static stretching was performed in three trials (10 s/trial).
All procedures described above were conducted in a clinical practice room at the university.
Data analysis
The normality of the data was assessed using the Shapiro–Wilk test. Repeated-measures analysis of variance was used for multiple ROM comparisons. An independent t-test was used to compare the ROM values between the HT and NoHT groups at each time point. Pearson’s correlation coefficient was used to measure the statistical relationship between lower-extremity flexibilities measured before stretching. Data analyses were performed using SPSS Statistics version 27 (IBM Corp., Armonk, New York, USA). Statistical significance was set at p < 0.05, and values are reported as mean ± standard deviation.
Results
A total of 32 young adults participated (mean age, 21.9 ± 2.3 years; mean height, 167.3 ± 8.1 cm; mean weight, 63.2 ± 12.2 kg). There were no significant intergroup differences in age, height, or weight (Table 1).
The WU did not significantly increase AKE in the HT (p = 1.000) or NoHT (p = 0.053) groups (Table 2, Figure 3). Post-WU, there was a strong negative correlation between AKE and ASLR (r = –0.844, p < 0.001) and a weak negative correlation between AKE and ADF (r = –0.373, p = 0.036). However, no significant correlation was noted between ASLR and ADF (r = 0.304, p = 0.091).
Table 1
Subjects’ characteristics
| Group | Age (years) mean ± SD | Height (cm) mean ± SD | Weight (kg) mean ± SD |
|---|---|---|---|
| HT (n = 16) | 22.2 ± 2.7 | 168.3 ± 8.1 | 61.9 ± 10.6 |
| NoHT (n = 16) | 21.6 ± 1.9 | 166.4 ± 8.2 | 64.6 ± 13.8 |
| p-value | 0.505 | 0.534 | 0.551 |
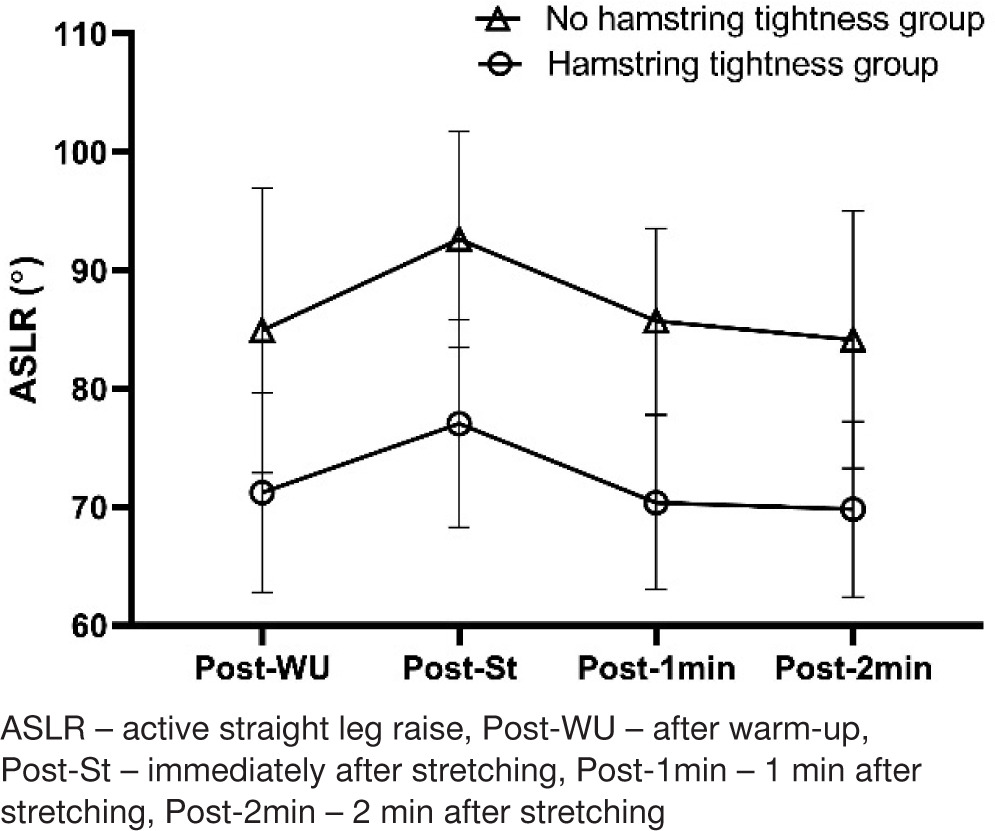
Diagonal stretching applied to the lower and upper body significantly increased mean AKE (p < 0.001) and ASLR (p = 0.001) in the HT group. However, in the NoHT group, stretching significantly increased AKE (p = 0.001), ASLR (p = 0.007), and ADF (p = 0.002) (Tables 3 and 4, Figures 4 and 5).
There were significant differences in AKE pre-WU (p = 0.001), post-WU (p < 0.001), post-St (p < 0.001), post-1 min (p < 0.001), and post-2 min (p < 0.001). There was also a significant difference in ASLR post-WU (p = 0.001), post-St (p < 0.001), post-1 min (p < 0.001), and post-2min (p < 0.001). However, there was no significant difference in ADF post-WU (p = 0.976), post-St (p = 0.579), post-1 min (p = 0.635), and post-2 min (p = 0.923). In ROM normalised to post-WU, there were no significant intergroup differences in AKE, ASLR, or ADF at post-St, post-1 min, and post-2 min.
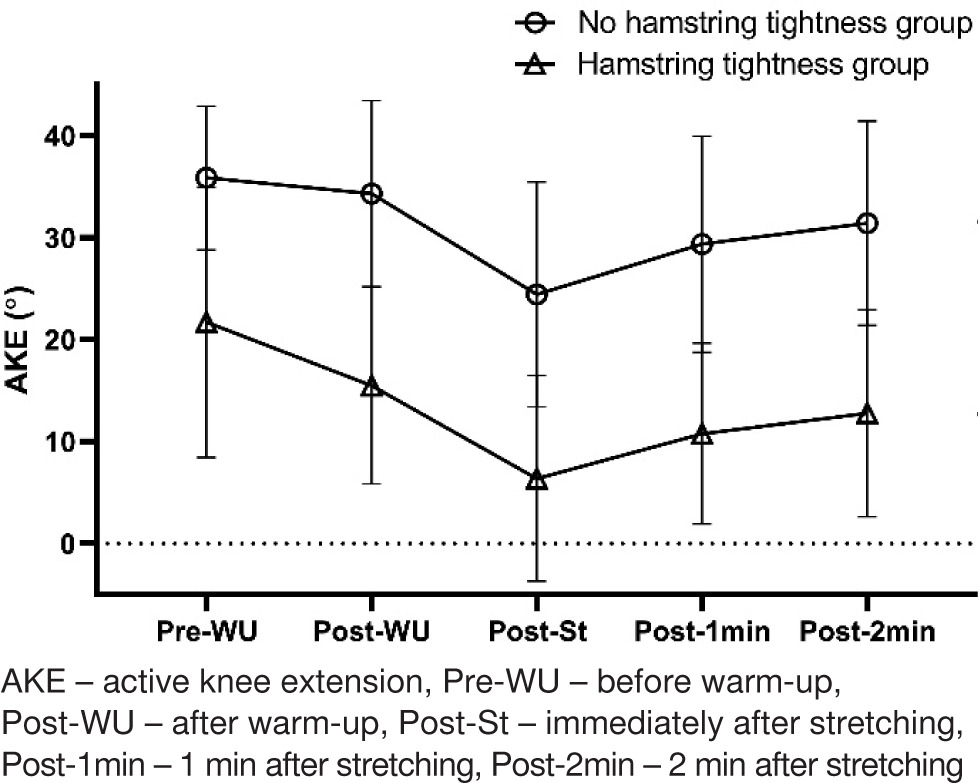
Table 2
Statistical analysis of active knee extension on repeated measurements
Table 3
Statistical analysis of active straight leg on repeated measurements
| Time | Post-WU | Post-St | Post-1min | |||
|---|---|---|---|---|---|---|
| HT | NoHT | HT | NoHT | HT | NoHT | |
| Post-St | 0.001 | 0.007 | – | – | – | |
| Post-1min | 1.000 | 1.000 | < 0.001 | 0.001 | – | – |
| Post-2min | 1.000 | 1.000 | < 0.001 | < 0.001 | 1.000 | 1.000 |
Discussion
The effect of a WU consisting of six trials of AKE on lower-extremity flexibility has been observed with some limitations. In the HT and NoHT groups, no statistical improvement in flexibility was seen after the WU. However, AKE at post-1 min was significantly different from that pre-WU, and while it was not significantly different compared to AKE at post-WU at 1 min after stretching, AKE returned to the post-WU level but did not reach the pre-WU level. This suggests that the elasticity of soft tissues allows them to temporarily lengthen, but they begin to return to their original length shortly after the external force is removed unless the tissue reaches the plastic deformation phase. Based on this, it can be indirectly inferred that the effects of WU were observed [30, 31]. Many studies conduct WU before stretching to avoid a cold start, which implies an expectation of a certain level of ROM increase after WU [16]. However, most of these studies did not measure flexibility before the WU. This is a limitation since it is difficult to determine the true effect of stretching without knowing an individual’s baseline flexibility. Spernoga et al. [18] performed six AKE trials. The first five trials were recognised as WU, while the sixth trial was defined as the baseline. However, because only post-WU flexibility was measured, the ability to clearly identify flexibility improvements caused by stretching is limited. If the WU contributes to an increase in flexibility to some extent, it is essential to be cautious about overestimating the effect of the intervention when pre-WU flexibility is not measured [32]. A previous study examining the longitudinal change in flexibility after stretching found that knee extension increased by approximately 6° from the first to the last trial [17]. Beyond a certain amount of time (< 5 min) after stretching, AKE returned to the value measured post-WU; after a longer period of time (> 5 min), it was lower than that measured post-WU [18, 33]. Therefore, it is necessary to confirm the definition of the baseline when interpreting experimental studies that have performed WU to avoid potential interpretation errors. Additionally, because individuals with no hamstring tightness showed marginal significance, it is important to be aware in clinical practice that the effect of WU may vary depending on an individual’s baseline flexibility.
AKE and ASLR were significantly different between the two groups at all measurement points (post-WU, post-St, post-1 min, and post-2 min). When the values measured at other points were normalised to the pre-WU values, no significant intergroup differences were noted. In other words, the intergroup difference in baseline flexibility was maintained even after stretching. This was similarly reported in a previous study in which both the hamstring tightness group (less than 80° PSLR) and the group with normal flexibility showed the same amount of flexibility increase after 12 weeks of active stretching [14]. Interestingly, in the present study, when examining longitudinal changes between the groups, some differences were observed. In the HT group, AKE at pre-WU was significantly different from that at 1 min post-WU. However, in the NoHT group, the AKE at pre-WU was significantly different from that after 2 min. This suggests that the increased flexibility due to stretching lasted longer in the NoHT group. Owing to the ceiling effect, it was expected that people with good flexibility would show a low level of flexibility improvement [34]. However, the actual results showed that the increase in flexibility was even greater, and the effect of stretching was maintained for a longer period. It is possible that the tensile force was insufficient to lengthen the tissues of those subjects with tightness during a single stretching session [35]. Tissues with relatively high flexibility may allow greater tissue elongation owing to their lower resistance to tensile force [36]. The decrease in resistance that occurs during stretching is linked to a decrease in muscle stiffness or an increase in muscle compliance [37]. In this study, similar phenomena were observed for ADF. In the NoHT group, there was a significant difference between ADF at post-WU and post-St, whereas there was no significant difference between them in the HT group. Another characteristic observed only in ADF was that there was no significant difference at baseline between the groups. The flexibility of the hip and knee can vary from person to person, but the flexibility of the ankle is not thought to be as high. Unlike ASLR and AKE, ADF has a separate characteristic, which is also reflected in the correlation verification [38].
The AKE and ASLR post-WU showed strong correlations. Furthermore, the trends in longitudinal changes in flexibility after stretching were similar. However, ADF showed a weak correlation with AKE and no significant correlation with ASLR. Although the correlation was weak, the significant relationship between ADF and AKE was likely due to their proximity. Anatomically, the knee and ankle are connected to a certain extent by passive connective tissue. This anatomical connection supports the observation that ankle position can affect knee joint kinematics. In a previous study that examined the effect of ankle position on the knee extension angle in a sitting position, ankle dorsiflexion significantly reduced knee extension [39]. During gait, when ankle motion was severely restricted using an ankle brace, the knee extension angle increased by 7.3° and dorsiflexion decreased by 9.5° [40]. In addition, ankle position is known to affect the kinematics of the knee joint, such as ROM, as well as its kinetics, such as torque [40–42]. In this study, although stretching was not directly applied to the tissues around the ankle, a significant improvement in flexibility was observed at the ankle because of the physiological and functional characteristics of the passive connective tissues mentioned above. This was also proven by the results of previous studies [43, 44].
Limitations
Flexibility before WU was measured only for AKE; ASLR and ADF were not assessed. Consequently, only a partial understanding of the WU’s effect on lower-extremity flexibility was achieved. Additionally, only the acute effects of stretching over a single session were confirmed, while the potential long-term benefits of repeated stretching remain unexplored. Future research should address these limitations by incorporating measurements of all flexibility parameters before WU and investigating the cumulative effects of longterm stretching protocols.
Conclusions
The HT and NoHT groups showed some similarities and clear differences in their responses to WU and stretching. The effect of WU on hamstring flexibility was limited but significant and maintained for a longer period in the NoHT group. There was no intergroup difference in the effect of stretching on ASLR. However, the effect of stretching on ADF was significant in the NoHT group but not in the HT group. ADF has characteristics that are distinct from those of AKE and ASLR. NoHT may respond differently to WU and/or stretching compared to HT in clinical practice.