Introduction
Currently, the population is ageing significantly, with the fastest increase projected for the ‘oldest’ old, and this has become a social phenomenon that will lead to changes both in older adults’ health and in society as a whole [1]. Considering that ageing has been related to physical, cardiorespiratory, and functional decline, and that there is a growing number of older adults reaching their 90s and 100s [2], the challenge is how to expand both the healthy and functional years in the life span.
Recently, the concept of successful ageing, based on a low probability of suffering illness or disability, great physical, functional and mental capacity, and an active commitment to life, has been studied [3]. Older adults who age successfully can maintain their functionality for longer and have lower morbidity and disability [4]. Therefore, it has become of paramount importance to understand and encourage successful ageing in older adults.
Moreover, it is crucial to focus on quality of life (QoL) in older adult groups, since it can help identify issues that are frequently linked to dysfunction, whether in the physical or mental domain [5]. For older adults, the concept of health-related QoL encompasses various dimensions, including physical health, mental state, levels of functionality, social interaction and context [6].
Physical activity can be a factor that significantly differentiates the average level of QoL for both middle-aged and older adults [7]. The level of physical activity also seems to play an important role, since a high practice of physical activity has shown to favour a functional capacity that can, in turn, guarantee the autonomy and independence in activities of daily life [8]. Moreover, physical activity can help older adults preserve cognitive function, delay dependency, and reverse frailty [9, 10]. Recently, a review has highlighted that walking can lead to improved lung function in healthy older adults [11]. In fact, inactive behaviour and sedentary lifestyles increase with age and are major risk factors for chronic health conditions [12].
In spite of this evidence, previous reports have shown that only 25% of individuals over 65 meet the recommended minimum activity levels for maintaining health [13]. This might be attributed to the impact of the ageing process on the health parameters of older adults. Firstly, it is well-documented that the decline in the musculoskeletal system’s capacities can result in weakness, frailty, reduced balance, diminished strength, and impaired functionality, among other issues [14]. Moreover, older adults have an increased incidence of painful conditions related to musculoskeletal, nervous system, or metabolic changes, with studies reporting between 25–76% of community-dwelling older adults suffering some type of pain [15]. Common musculoskeletal conditions in older adults include neck pain, primary headaches, and shoulder discomfort [16]. Previous literature has stated that older adults might have different views and understandings of pain compared to younger adults, but the ideal source of pain history is the patient (self-report) [16].
These changes not only affect skeletal muscles but also the cardiorespiratory system undergoes a series of slow and progressive morphological and functional modifications with the ageing process [17]. All these changes and conditions have a strong impact on older people’s health-related QoL, which has been shown to decline with advancing age and to be reduced among inactive older adults with diminished physical performance [18]. However, no previous study has focused on how being physically active and ageing parameters such as pain, balance, cardiorespiratory or functional ones can influence and explain how to have a successful QoL. Therefore, less focus has been given to comprehensively understanding factors related to QoL in successful and active older adults. All considered, physical, cardiorespiratory, and functional abilities, parameters that are all so intricately affected with ageing, could be enhanced and have, in turn, a strong influence on achieving a successful and active ageing, and could make a profound effect on older adults’ health and QoL. Thus, to explore complex relationships and make forecasts by examining how these multiple factors influence QoL, a multiple regression analysis should be applied. The hypothesis of this study was that successful older adults who are physically active will have positive health parameters, and these will influence their QoL.
Therefore, the aim of this study was to describe and analyse QoL, physical activity, musculoskeletal pain, balance, cardiorespiratory and functional characteristics of older adults over 60 years of age, who comply with the concept of successful ageing. It also aimed to analyse the possible associations between physical and mental health-related QoL and physical, cardiorespiratory and functional health indicators.
Subjects and methods
Design
A cross-sectional study was performed at the Laboratories of the University of Valencia (Spain) from February to April 2021. Participants were assessed once by a physiotherapist. The manuscript was written in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) protocol [20].
Participants
Participants were recruited from older adults’ associations of Valencia (Spain). A non-probability sampling approach was used to select the study participants. Inclusion criteria were: community-dwelling older adults (considered as those of over 60 years of age [21]); with successful ageing, defined as those who had not suffered stroke, coronary artery disease, angina, acute myocardial infarction, cancer, or diabetes; plus they had optimal cognitive, physical, mental, respiratory and vascular function and a lack of disability while being functionally independent [22]; and considered as active by the International Physical Activity Questionnaire (IPAQ) short version [23]. Exclusion criteria were: Mini-Mental State Examination < 25 points (administered by a trained interviewer) and suffering any acute injury (acute musculoskeletal or osteoarticular pain).
Outcomes
All participants undertook a face-to-face assessment performed by a physiotherapist with more than 10 years of experience that included:
Anthropometric variables: age, sex, body weight (kg) measured by a Tanita BC 601 weighing device (TANITA Ltd., Tokyo, Japan), and height (cm) measured with a stadiometer SECA 213 (Seca Ltd., Hamburg, Germany), with both instruments having been shown to be reliable and valid for use in community assessments [24]. Also, body mass index (BMI) was calculated (kg/m2).
Primary outcome
Quality of life: The Short Form 12 (SF-12) Health Questionnaire v2 was used, which measures the impact of health on everyday life. It consists of 12 items that include areas related to physical and mental aspects of health, thus determining a physical subscale and a mental subscaleusing data from the Medical Expenditure Panel Survey longitudinal panel (2014–2015. The maximum score that can be obtained is 100 points, which indicates the highest level of health. It is a reliable and valid instrument with high internal consistency for both physical and mental components (Cronbach’s alpha: 0.87 and 0.86, respectively) and good and moderate test-retest validity (intraclass correlation coefficient (ICC): 0.79 and 0.59, respectively) [25].
Secondary outcomes
Physical activity variables: (1) Level of physical activity, calculated by the number of METs/week, and then classified accordingly (moderate-intensity, level 2, and high-intensity, level 3) by the International Physical Activity Questionnaire (IPAQ) short version [23]; (2) Number of days per week participants exercised; (3) Type of exercise; (4) Perception of exercise, benefits and barriers, using the Exercise Benefits/Barriers Scale (EBBS), composed of 43 items evaluated using a 4-point Likert scale (‘completely agree’ to ‘completely disagree’); the higher the score, the more positive the perception of exercise. The reliability coefficient (Cronbach’s alpha) is 0.95 for the total scale [26].
Musculoskeletal pain: patients were asked if they felt musculoskeletal pain and to rate the intensity of this musculoskeletal pain intensity with the Visual Analogue Scale (VAS). The VAS is a unidimensional measure of non-specific perceived pain intensity that is appropriate for use with older adults [27]. It is a continuous scale composed of a horizontal line typically 10 cm in length, on which the participant is asked to indicate pain intensity with a score of 0 being ‘no pain’ and 10 being ‘the worst pain imaginable’, a higher score indicates greater pain intensity. Participants were asked to indicate the body area that was most painful and to rate the intensity of the ‘current’ pain or pain intensity ‘in the last 24 hours’ for that area, the VAS has a high internal consistency (0.97) [28]. Also, an ad hoc question was asked with a yes/no answer indicating the need of medication and/or visiting a physiotherapist for this pain.
Balance: (1) Static balance, measured by two variables: Static balance, with the Unipedal Stance Test (UPST) which consists of assessing the time the participants can maintain eyes closed monopodal support while their arms are crossed at chest level and one leg is raised [29]. Three repetitions were done, and the best was selected for analysis. This test has shown an ICC of 0.998 for eyes closed [29]. (2) Dynamic balance was assessed with a variant of the Star Excursion Balance Test (SEBT), the Lower Quarter Y-Balance Test (YBT-LQ) which is a reliable and valid measure (ICCs for intratester reliability 0.78–0.96 and ICCs for intertester reliability were 0.35–0.84) [30]. Participants have to maintain stability while moving one lower limb in three directions (anterior, postero-lateral and posteromedial) and keeping the other limb stable. For the analysis, the mean of three attempts in each direction was recorded [31]. A principal component analyses was performed to summarise the three directions of the right leg in one variable and the three of the left leg in another variable.
Cardiorespiratory variables: (1) Pulse oximetry: Oxygen saturation (SpO2) and heart rate were assessed with a pulse oximeter, SmartOx (WEINMANN, Medical Technology, Hamburg, Germany). Oxygen saturation has shown to be a reliable method for detecting hypoxaemia and has been reported accurate in reflecting one-point measurements of SpO2.(2) Forced spirometry using a spirometer Spirovit SP-10 (Contec, Barcelona) was performed according to American Thoracic Society standards. Dynamic lung volumes such as forced vital capacity (FVC) and the forced expired volume at 1 second (FEV1) were obtained by the forced expiratory flow manoeuvre, and the FEV1/FVC ratio was calculated. For FVC and FEV1, an 80% or over is an optimal value [32], and for the FEV1/FVC ratio, a decreased percentage defines the concept of ‘obstruction’. Spirometry has shown an ICC of 0.89 in COPD patients [33].
Functional variables: (1) The Six-Minute Walk Test (6MWT), which aims to walk for 6 minutes around the 30 m distance between cones. Pulse oximetry, final heart rate, SpO2, and dyspnoea were recorded using the Borg scale. The 6MWT is a reliable measure (ICC = 0.82–0.99) [34]; (2) Timed Up and Go test (TUG), where participants had to stand up from a chair, walk a 3 m distance, turn around and walk back, and sit back on the chair. The test is repeated 3 times and then the mean is calculated (i.e. < 10 Independent Mobility, 10–20 Mostly Independent, 20–29 variable mobility, > 30 reduced mobility [35]). It has shown excellent interrater reliability and varied intrarater reliability [36].
Sample size calculation
G*Power version 3.1.9.7 was used to calculate the sample size for the linear multiple regression analysis. Five predictor variables were established, along with a medium effect size (f2 = 0.15), a type I error ( ) of 5%, and a type II error ( ) of 20%, according to a previous study conducted by Wanderley et al. [37]. The findings suggested that 92 people would be needed for the sample.
Statistical analysis
Statistical analyses were carried out through the SPSS program (v. 25, SPSS Inc., Chicago, IL, USA). Normality of variables was assessed using the Shapiro–Wilk test. Levene’s test assessed homoscedasticity. Data are shown as mean and standard deviation (SD) for continuous variables, and frequency and percentage for categorical ones. As the assumption of normality was fulfilled in the variables analysed, correlations between dependent and independent variables were analysed using the Pearson coefficient (0.10–0.29 values indicated a small effect, 0.30–0.49 moderate effect, and ≥0.50 large effect). The all-bivariate correlation was displayed using a Pearson correlation heatmap in the Matlab software (Matlab 2023, Mathworks, Natick, MA, USA). The correlation heatmap is a graphical representation in which each variable is depicted by a row and a column, and the cells within the matrix display the correlations between them. The colour intensity in each cell is a key indicator of the magnitude and direction of the correlation. Darker hues indicate stronger correlations, while lighter colours indicate weaker correlations. Positive correlations (when one variable increases, the other variable tends to increase) are represented by a warm colour (red). Negative correlations (when one variable increases, the other variable tends to decrease) are represented by a cool colour (blue). The potential of respiratory and functional factors to predict the variability of physical and mental health was investigated using a multiple stepwise linear regression model. Coefficient (B), standardised beta coefficients ( ), R2,adjusted R2, and p-values were used to assess the association’s strength. Only the five independent variables with the highest Pearson correlation coefficient values were included in a prediction model, based on the results of the correlation test. The significance level was chosen at p < 0.05.
Results
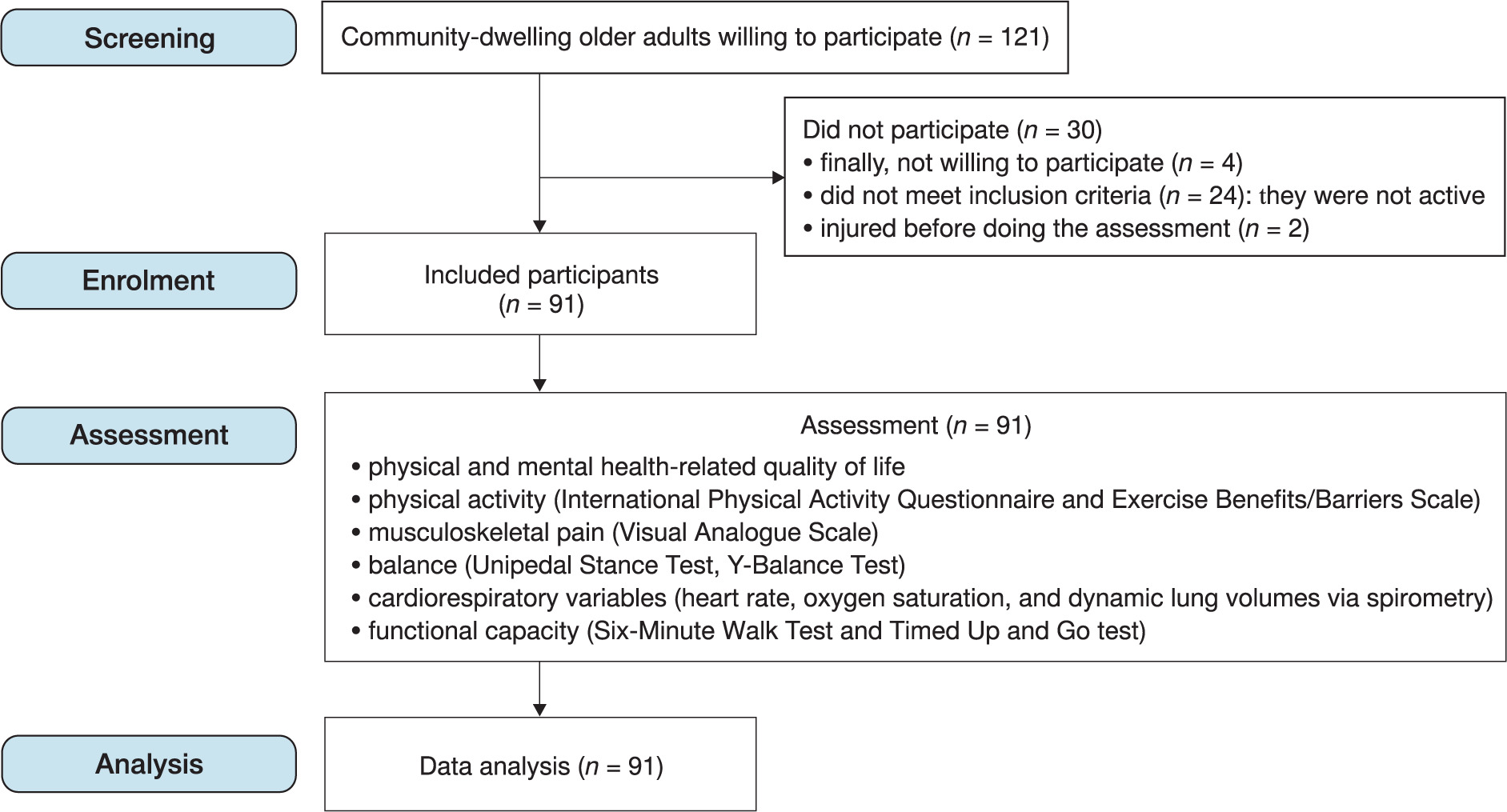
Of the 121 initial participants, in the end, a total of 91 older adults met the inclusion criteria and were analysed. Thirty participants were excluded for not being willing to participate, not meeting the inclusion criteria or being injured prior to assessment. No adverse events were reported (Figure 1).
Participants had a mean (SD) age of 69.18 (5.08) years, with 70.33% being women. All participants exercised regularly, and nearly 80% performed this exercise with moderate intensity. Anthropometric and physical activity characteristics are shown in Table 1.
Table 1
Anthropometric and physical activity variables of the sample.
QoL, musculoskeletal pain, balance outcomes (i.e. UPST, YBT-LQ), cardiorespiratory outcomes (i.e. heart rate, SpO2,FVC, FEV1, and FEV1/FVC), and functional outcomes (i.e. 6MWT and TUG) are shown in Table 2. The 6MWT, heart rate, SpO2 and dyspnoea parameters before the test were adequate and those registered after the test are shown. Regarding pain, 93.41% of the sample had musculoskeletal pain, and the pain intensity was 4.31 (SD = 2.36). Pain was distributed in different areas with the lumbar spine being the area where more participants had pain (8.13%), followed by head and/or neck pain (60.44%), knee pain (56.04%), dorsal spine (30.77%), shoulder pain (30.77%), hip and pelvic pain (29.67%) and ankle and/or foot pain (28.57%) (Supplementary material 1). A total of 32.25% took medication for the pain, and 77.50% regularly visited a physiotherapist with the aim of relieving pain.
Table 2
Pain, balance, respiratory, and functional outcomes, and quality of life of the sample
[i] Descriptive analyses were performed. VAS – Visual Analogue Scale, HR – heart rate, SpO2 – saturation of peripheral oxygen, FVC (l) – forced vital capacity, FEV1 – forced expiratory volume in one second, UPST – unipedal stance test, YBT-LQ – Lower Quarter Y-Balance Test, 6MWT – Six-Minute Walk Test, TUG – Timed Up and Go, SF-12 – Short Form 12 Health Survey
Correlations and regression models
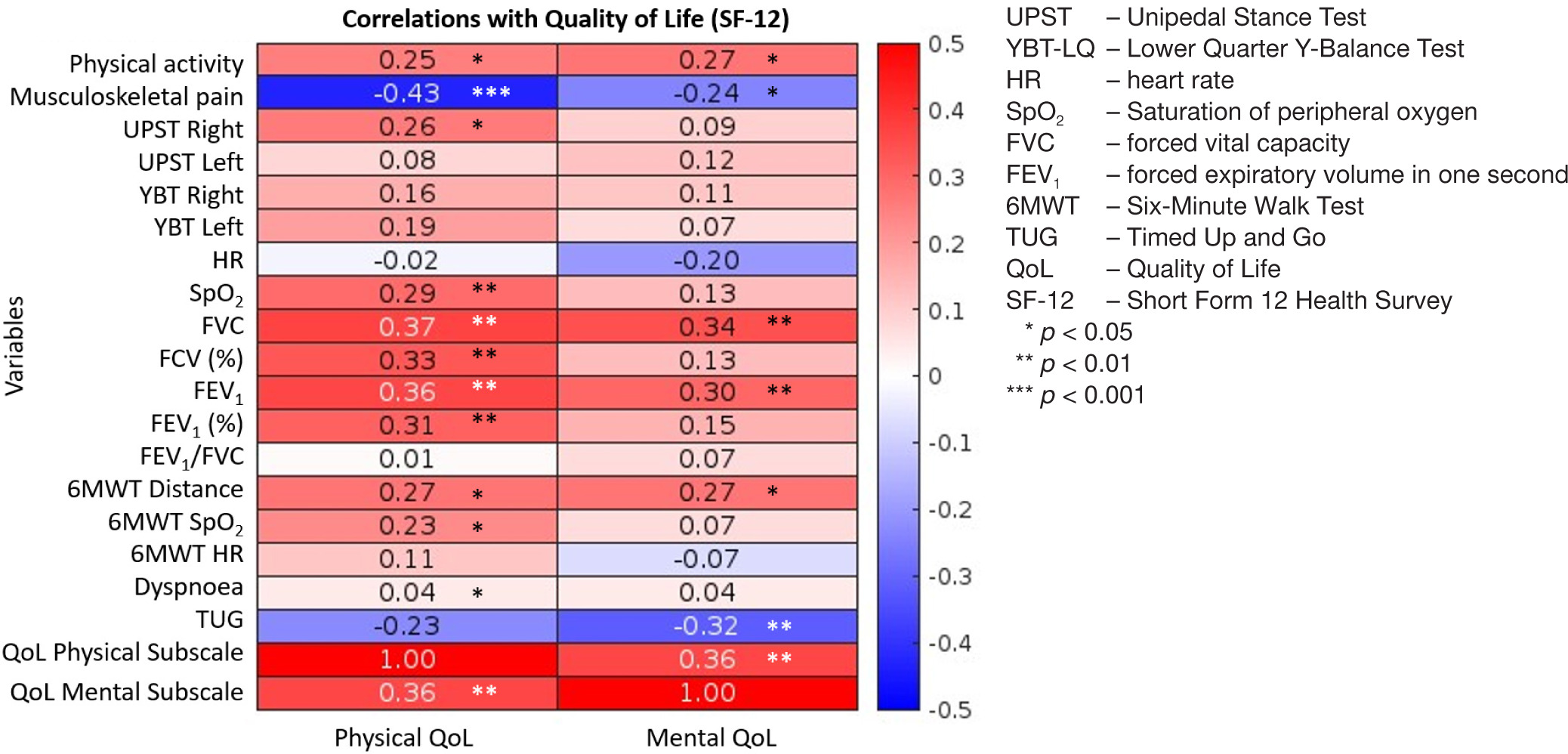
The Pearson Correlation Coefficient showed a statistically positive correlation between both physical and mental health-related QoL and higher levels of physical activity (r = 0.25, p < 0.05; and r = 0.27, p < 0.05, respectively) (Figure 2, and Supplementary material 2). Moreover, both physical and mental health-related QoL showed a statistically negative correlation with pain; so, the higher the pain, the lower the QoL. Physical health-related QoL showed a positive association with cardiorespiratory variables (SpO2, FVC, and FEV1) static balance (UPST), functional parameters (6MWT distance and SpO2 at the end of the test, and the TUG), and the mental health-related QoL. As for mental health-related QoL, it showed positive correlations with respiratory variables (FVC, and FEV1), functional parameters (6MWT distance and the TUG), and physical health-related QoL.
Figure 2
Correlation analyses were performed. Correlation heatmap between physical and mental health-related quality of life and the secondary outcomes (i.e., physical activity, musculoskeletal pain, balance, cardio-respiratory variables and functional variables). Darker colours indicate stronger correlations, while lighter colours indicate weaker correlations. Positive correlations (when one variable increases, the other variable tends to increase) are represented by a warm colour (red). Negative correlations (when one variable increases, the other variable tends to decrease) are represented by a cool colour (blue)
For the regression analyses, only variables with significant correlations concerning physical health-related QoL and mental health-related QoL were considered (Table 3). For physical health-related QoL, the model showed an R2 of 0.26, meaning that 25.90% of physical health variability was related to musculoskeletal pain and FVC (F(2,84) = 14.68, p < 0.01). For mental health, the model shows an R2 of 0.19, indicating that 19.10% of mental health variability was related to physical health and TUG (F(2,84) = 9.89, p < 0.01).
Table 3
Multiple stepwise linear regression analysis for quality of life in relation to mental and physical health
[i] Multiple stepwise linear regression analyses were performed. B – regression coefficient, – standardised coefficient, VIF – variance inflation factor, SEE – standard error of estimate, SF-12 – Short Form 12 Health Survey, VAS – Visual Analogue Scale, FVC – forced vital capacity, FEV1 – forced expiratory volume in one second, TUG – Timed Up and Go * p < 0.05
Discussion
Our results showed that successful and active older adults tend to exercise with moderate physical activity, with walking 2–3 times a week being the most common physical activity. Globally, their mental health-related QoL was higher than the physical, and 93.41% of the sample had musculo-skeletal pain. Their cardiorespiratory parameters are adequate, and they have optimal functional independence. Their physical health-related QoL is significantly associated with musculoskeletal pain and cardiorespiratory parameters such as FVC. Mental health-related QoL is significantly related and can be predicted by adequate physical health-related QoL and good performance in the TUG functional parameter. Therefore, the overall QoL of successful and active older adults can be influenced by their respiratory conditions and their functional capacity; thus, these are areas healthcare professionals should focus on to improve QoL in the older population.
New disease patterns of older people have risen due to sedentary lifestyles, a lack of physical activity, stress, poor diets and consumption of toxic substances [38]. Comprehensively investigating, like in this study, which parameters favour a good QoL in people with successful ageing, allows clinicians to take them into account in practice, which could reduce the costs caused by ageing in primary care consultations as well as in the health system in general, both in terms of physical and psychological repercussions.
Physical health-related quality of life
Our results showed that physical health-related QoL is significantly associated with optimal levels of FVC. This may be explained because ageing is characterised by a reduction in muscle strength, joint mobility and cardiorespiratory capacity, and this reduction in physical capacities translates into greater breathing effort and a decrease in respiratory values. Moreover, there is a decline in lung function FVC, FEV1, and peak expiratory flow rate as age increases [39]. Our participants, by having a successful ageing process and an active life, showed optimal spirometric results [40], with mean FVC and FEV1 very close to 80% (82.18 and 79.85%, respectively) and a FEV1/FVC of 78.18%. Our results highlight the importance of monitoring these variables in older adults, since they have shown a relationship with physical health-related QoL, which is ultimately one of the main objectives of geriatric healthcare. Furthermore, respiratory symptoms, frailty, and mortality are strongly associated with respiratory impairment [41]. Since respiratory parameters are feasible, simple and cost-effective to monitor through spirometry [32], it is important for health professionals to make use of these tools, so that preventive and treatment measures can be taken to achieve or maintain optimal levels. It should be noted that physical activity is a viable strategy for improving cardiorespiratory function [42], which also provides benefits in different physical, social and psychological dimensions [43]. Thus, promoting physical activity will improve their cardiorespiratory function, which in turn will enhance their physical health-related QoL.
In addition, our results showed that pain is another predictor of physical health; thus, higher levels of pain intensity tend to be associated with lower QoL. Chronic pain can have a significant impact on physical function, emotional well-being, and overall enjoyment of life, particularly in older adults, who may have other age-related health problems [44]. Therefore, it is important to manage pain effectively through individually tailored therapeutic approaches such as physiotherapy.
Mental health-related quality of life
Regarding mental health, our study has corroborated the relationship between physical and mental health-related QoL. According to the World Health Organization, more than 20% of people over 60 years old suffer from some type of mental disorder, with depression and dementia being the most prevalent. 3.8% of the older population is affected by anxiety disorders [45], commonly treated with antidepressants, but these may produce cardiovascular problems, epilepsy and an increased risk of mortality [46]. This makes it necessary to look for other alternatives, such as being active and practicing regular physical activity. Our results showed that functional capacity in terms of the TUG is associated with mental health. This is consistent with previous studies [47], which found that older adults with poorer mental health presented poorer performance on the TUG. In clinical practice, it is very interesting to be able to monitor functional capacity using the TUG, as it is a simple tool to use and offers vast information [48]. This in turn will make it possible to develop individualised prevention and treatment strategies for older adults.
Moreover, poor endurance and energy have an effect of 13.4% on the mental-health QoL [49]. In contrast, older persons who engage in more physical activity and have greater functional ability may be more resilient to anxiety and depression [50], and those with better functional capacity usually present higher vitality [37]. Interestingly, people with poor dynamic balance, functional mobility and gait as well as depressive symptoms often have a fear of falling [51], which may lead to a sedentary lifestyle. Our results also showed some correlations between balance variables and physical-health QoL; however, they were not significant in the predictive model, probably due to the need for a larger sample.
Future research directions
Our results, together with previous studies that highlight that exercise programs for older adults can reduce healthcare costs and prevent falls, strokes, heart attacks, and chronic diseases [10], enhance the idea of promoting research related to physical activity in older adults. Moreover, ageing is a complex process that must be conceived as a whole, which is in line with showing a relation between physical and mental health, so a multicomponent approach should be taken into consideration in future research.
Applications of the findings
Overall, improving respiratory, physical and functional variables may favour an active and successful lifestyle in older adults and enhance mental and physical health-related QoL. These findings are of interest for identifying risks and protective factors that favour successful ageing and developing strategies not only for prevention and treatment but also for promoting successful and active ageing in society.
Limitations
The sample consisted mainly of women, either because this is a situation that is a common characteristic to older adults of the population in Spain, or because women were more willing to collaborate. Thus, greater equality regarding sex would be important in future research. Additionally, although the sample size calculation indicated the need for 92 participants, only 91 individuals were ultimately included, which may slightly reduce the statistical power of the analyses and should be considered when interpreting the results. Future research would also benefit from a bigger sample size or even from analysing gender differences.
As strengths, this study includes a set of variables in active older adults with successful ageing that have not been previously studied or contrasted in relation to their impact on QoL. Therefore, this study confirms the common idea that physical activity is related to health parameters relevant to an optimal QoL.
Conclusions
Older adults with successful ageing who perform physical activity have optimal health parameters, and these parameters show relationships between them. Respiratory conditions and functional capacity have shown to influence the physical and mental health-related QoL of successful active older adults. Thus, these are areas healthcare professionals should focus on to improve QoL in the older population.