Introduction
Menopause is defined as the period in a female’s life during which the ability to procreate ceases, marking the end of menstrual cycles. According to the World Health Organization (WHO), menopause is described as the permanent termination of the menstrual cycle in females, brought on by the decline of ovarian follicular activity. Natural menopause occurs when there is an unusual 12-month span in which there is no menstruation without any known physiological or pathological cause [1].
Between the ages of 40 and 55, females see a sharp drop in the levels of oestrogen and progesterone, which causes a number of physical and somatovegetative symptoms. This phase of hormonal fluctuations is termed perimenopause. Itis defined by the WHO as the year that follows menopause and the time immediately before it. It is sometimes referred to as the menopausal transition, when a female’s body naturally enters menopause. In India, females typically go through menopause at age 48. Both the physical and mental symptoms are a result of a natural process. Although there is no need for therapy, it can assist in reducing the symptoms. The Staging of Reproductive Ageing Workshop (STRAW) staging system has subdivided perimenopause into 3 stages:
Perimenopause might start 8 to 10 years before the onset of menopause. Menstrual abnormalities are an early indicator of the progression of menopause, which can appear in a female in her early 40s. The female sex hormones, progesterone and oestrogen, rise and decline in different proportions. Menstruation without ovulation results from the lengthening or shortening of the menstrual cycles. This cycle continues until menopause, or until the ovaries cease producing and releasing eggs. In the final 1–2 years of the menopausal transition phase, i.e. perimenopause, there is an acceleration of the oestrogen level declining as menopause approaches [3].
During the perimenopause phase, females can have a wide range of symptoms. Vasomotor symptoms include palpitations, headaches, sleep difficulties, night sweats, and hot flashes. Psychological symptoms include impatience, anxiety, mood fluctuations, depression, lack of concentration, and forgetfulness. Problems related to the urogenital system include painful sex, low libido, and dry vagina. Skin issues include brittle nails, dry skin, and dry hair. Additional symptoms include increased weight, a decrease in bone mass, and aches and pains in the muscles and joints. Among all these signs and symptoms, restlessness in sleep is the most prevalent sign (51.7%) [3, 4].
Insomnolence, also known as sleep disruption/insomnia, ranks among the most prevalent concerns in the menopausal transition phase. Perimenopausal females usually neglect the symptoms of insomnia as an indicator of a sleep disorder and may acknowledge sleep disruptions as typical, and as a result not seek treatment [3].
In the past few years, the use of hormone replacement therapy (HRT) has increased to treat the menopausal manifestations among females. Although it has been useful in addressing climacteric symptoms, it is not considered an appropriate treatment option as it involves risks that include coronary heart disease (CHD), pulmonary embolism, breast cancer, and stroke.
To prevent these serious adverse effects of HRT, multiple therapeutic treatment options have been used, which include yoga, aerobic exercises, mindfulness meditation and progressive muscle relaxation.
Yoga is an age-old discipline that develops the body, mind, and spirit through a harmonising system. It is a traditional Indian body-mind discipline that enhances both physical and mental well-being through postures, mindful breathing, meditation, and guided imagery. Yoga is a mental workout that improves brain function by restoring the body’s circadian rhythm, which in turn helps to calm the mind. A regular yoga routine improves the quality of life by lowering the frequency of nighttime awakenings [1].
For females undergoing the menopausal transition phase, walking helps to stabilise the cyclic fluctuations of oestradiol (oestrogen), which in turn helps to reduce menopausal symptoms [1, 2].
Treadmill walking and yoga therapy are two of the non-pharmacological alternative therapies that have been researched as effective ways to manage climacteric symptoms without having any negative effects.
Subjects and methods
Participants
The study was carried out on 40 perimenopausal females. The selection of participants met the following requirements: females aged between 40–55 years; females experiencing climacteric symptoms like hot flashes, insomnia/sleep disturbances and further modifications that could worsen social or personal relationships and lower one’s quality of life overall; perimenopausal females with amenorrhoea for at least 3 months but less than 12 months or irregular periods; Pittsburgh sleep quality index score 5 and above; Insomnia severity index score 8 and above; subjects who can read and understand English and Hindi. Females who met the following requirements were excluded: females undergoing HRT; females who have been doing yoga for a month or longer, or who exercise more than twice a week for at least half an hour each time; subjects who have surgically or medically induced menopause; history of any diagnosed psychiatric illness and taking psychiatric medication; history of any musculoskeletal conditions that may hamper the practice sessions of yoga therapy; females with uncontrolled hypertension (140–159/ 90–99 mm Hg) or diabetes mellitus (random BSL > 200 mg/dl) which may affect the vasomotor symptoms; females diagnosed with Hypothyroidism or Hyperthyroidism; pregnancy.
Randomization
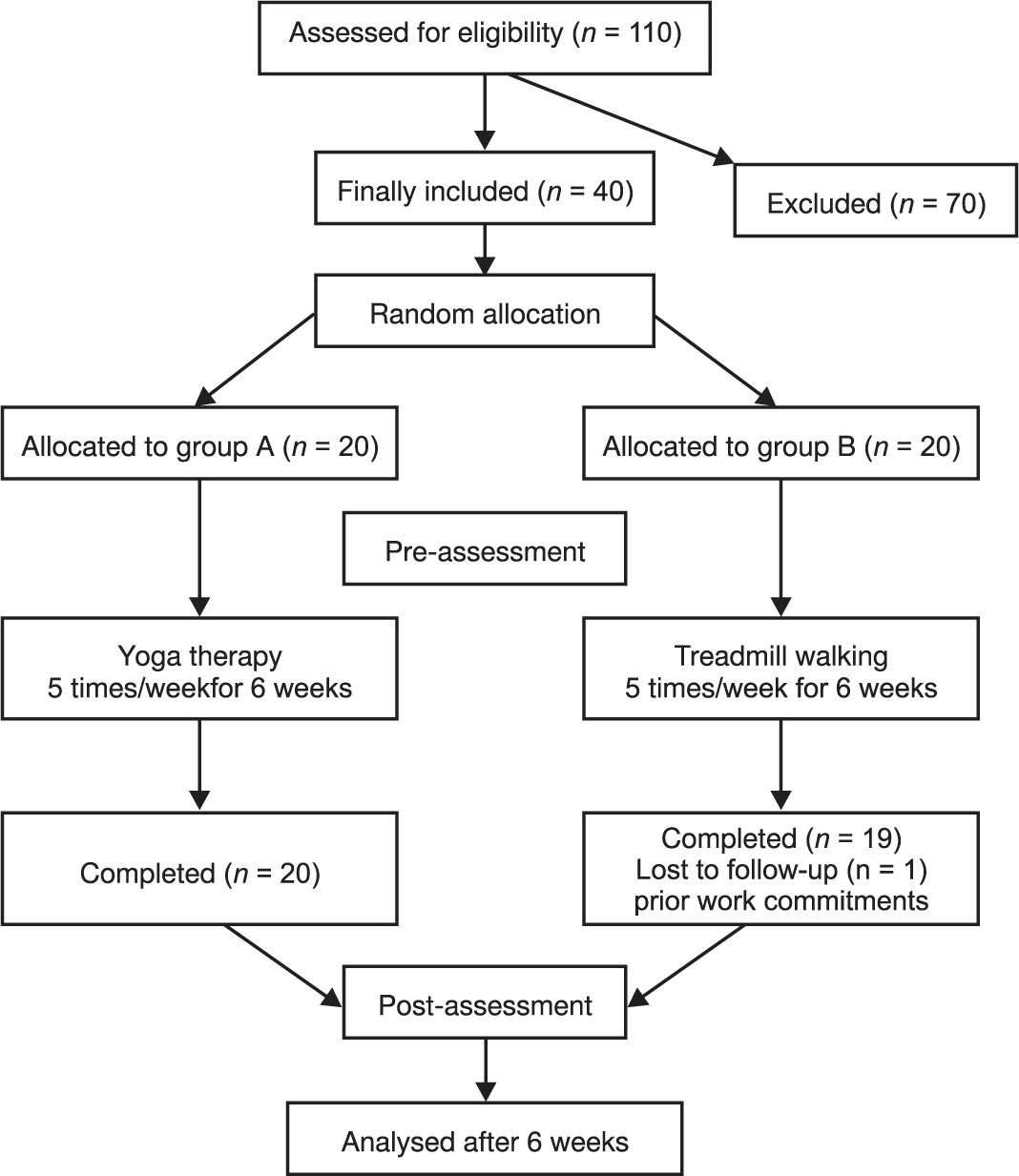
The subjects were sorted using a computer-generated random allocation algorithm into two groups: group A (yoga therapy, n = 20) and group B (treadmill walking, n = 20) (Figure 1).
Intervention
The interventions were carried out for six weeks, five days a week, under supervision. Each session was divided into three sections: a warm-up, a yoga or treadmill walking program, and a cool-down. For the duration of the session, the participant was accompanied to ensure their safety. The sessions were terminated whenever any of the termination criteria (breathlessness, giddiness, angina, any musculoskeletal injury taking place during the intervention) occurred.
Procedure
Study commenced after receiving ethical clearance of institutional ethical committee, Selection of participants was done according to the inclusion and exclusion criteria. Written informed consent was obtained from patients. Sheets with demographic information were completed. The interventions were carried out for six weeks, five days a week, under supervision.
Each session as shown in Table 1 was divided into three sections: a warm-up, a yoga or treadmill walking program, and a cool-down. At the end of the 6-week intervention, the demographic data and outcome measures Pittsburgh Sleep Quality Index (PSQI), Menopause Rating Scale (MRS), Insomnia Severity Index (ISI), Menopause-Specific Quality of Life Questionnaire (MENQOL) for the post-test values were assessed, and all measurements were recorded.
Table 1
Exercise protocol
Outcome measure
– Pittsburgh Sleep Quality Index (PSQI): A validated tool to assess sleep quality and disturbances, consisting of 19 self-rated items forming 7 components (score range 0–21), with higher scores indicating poorer sleep quality (Cronbach’s = 0.87).
– Insomnia Severity Index (ISI): A 7-item scale evaluating the severity and impact of insomnia, with total scores ranging from 0–28 and categorized from no insomnia to severe insomnia (Cronbach’s = 0.84).
– Menopause Rating Scale (MRS): An 11-item self-administered scale assessing menopausal symptoms across psychological, somato-vegetative, and urogenital domains, with total scores ranging from 0–44 (Cronbach’s = 0.84).
– Menopause-Specific Quality of Life Questionnaire (MENQOL): A 29-item self-administered questionnaire assessing menopause-related quality of life across vasomotor, psychosocial, physical, and sexual domains, rated on a 0–6 scale (Cronbach’s = 0.81).
The intensity of walking was measured using the rate of perceived exertion (Borg’s scale). The first three weeks of the study involved the participants walking at a level that corresponded to 11–13 (light to moderately hard) on the 6–20 scale. From week three to week six, the participants were told to walk at a level that matched 13–15 (somewhat hard to hard) on the 6–20 scale.
Statistical analysis
Data were analysed using the statistical package SPSS 26.0 (SPSS Inc., Chicago, IL) and the level of significance was set at p < 0.05. Descriptive statistics were performed to assess the mean and standard deviation of the respective groups. The normality of the data was assessed using the Shapiro–Wilk test. Inferential statistics to determine the within-groups difference were calculated using a paired t-test, and the between-groups analysis was performed using an independent t-test.
Results
Table 2 shows the baseline demographic data of the participants. Table 3 shows participants’ clinical details for outcome measures (PSQI, ISI, MRS, and MENQOL), presented as mean ± SD for pre- and post-intervention assessments.
Table 2
Baseline demographic data of the participants
Table 3
Within and between group analysis of outcome measures
Statistically significant within-group improvements were observed for both interventions across all outcomes (p = 0.0001). Between-group differences were significant for insomnia severity, menopausal symptoms, and menopause-specific quality of life, favouring yoga therapy, but not significant for sleep quality.
Discussion
This study compared the benefits of yoga treatment and treadmill walking on quality of life and insomnolence in females going through menopause. In our study, Table 2 the average age of those receiving yoga treatment (group A) was 46.75 ± 4.82, and the treadmill walking group (group B) had a mean age of 45.15 ± 3.15. The study’s conclusions showed that yoga treatment outperformed treadmill walking in terms of optimising life in general and sleep quality in particular.
One of the major benefits of yoga is attaining mental peace and fostering feelings of wellbeing, relaxation, increased self-assurance, enhanced efficiency, better sleep quality, reduced irritation, enhanced concentration, and a positive view on life. Yoga produces balanced energy, which is essential for the immune system to work properly. The posterior, or sympathetic, region of the hypothalamus is inhibited by yoga. This inhibition restores the autonomic regulating reflex mechanisms linked to stress and maximises the body’s sympathetic reactions to stressful stimuli. By stimulating the rewarding pleasure centres in the middle forebrain and other places that contribute to a sense of ecstasy and pleasure, yogic activities suppress the areas that are responsible for fear, aggression, and fury. Among individuals who practice yoga and meditation, this inhibition leads to reduced levels of anxiety, depression and irritability and improves sleep efficiency, thereby improving the quality of life [5]. Our study’s findings support those of Catherine Woodyard’s investigation [5], which found that yoga enhances the body’s circadian rhythm and helps to relax the mind, which in turn improves sleep and, ultimately, quality of life.
Physical activity is essential for overall health and well-being. It is essential for maintaining a healthy weight, boosting vitality and strength, elevating mood, lowering the risk of illness and injury, and encouraging deeper sleep. The quality of life can also be improved through regular exercise. People who exercise have more emotional balance and a more positive self-image. Exercise promotes the release of endogenous morphine’s, also known as endorphins, which are feel-good chemicals that induce a calming and blissful state. Studies have shown that walking can significantly improve one’s mental health and standard of living. In comparison to inactive females in perimenopause, physically active perimenopausal females do not appear to have as many sleep problems, memory loss, hot flashes, joint aches and stiffness, or digestive problems [6].
Forty perimenopausal females, aged 40 to 55, were split into two groups for this experimental study: Group A received yoga treatment (n = 20) while group B walked on a treadmill (n = 20). The Pittsburgh Sleep Quality Index, Insomnia Severity Index, Menopause Rating Scale, and Menopause-Specific Quality of Life Questionnaire were employed to assess the general quality of the participants’ sleep and life.
Oestrogen and progesterone levels rapidly drop in females between the ages of 40 and 55, leading to a variety of physical and somato-vegetative symptoms. Perimenopause is the word used to describe this stage of hormone changes. Perimenopause may begin 8 to 10 years before menopause. Menstrual irregularities can occur in a female in her early 40 s and are a good early sign of menopause’s advancement. Progesterone and oestrogen, the female sex hormones, rise and fall in varying quantities. The menstrual periods might prolong or shorten, resulting in menstruation without ovulation. This cycle continues until menopause, or until the ovaries stop releasing eggs. The oestrogen level declines more quickly as menopause approaches during the last one to two years of the menopausal transition phase, or perimenopause [7].
Aspects including height, weight, body mass index, and irregular menstruation patterns were also evaluated in our study. Table 3 shows that the Independent T-test’s group analysis of all the components showed no statistically significant results.
Booth-LaForce et al. [8] carried out a pilot study on Hatha Yoga therapy for problems related to menopause. It was a 10-week study with a 75-minute yoga session5 days each week. They assessed a variety of menopausal symptoms, of which sleep disturbances or insomnia was one. They used a variety of postures, breathing exercises and relaxation techniques specifically used for menopausal symptoms. The sleep disruptions were evaluated using the Pittsburgh Sleep Quality Index. There is some evidence that yoga improves the waking alpha activity in the brain, which is a sign of relaxation, and lowers autonomic arousal. Nonetheless, there is mounting evidence that menopausal sleep disturbance may have a different aetiology than the hot flashes that occur throughout the night, calling for targeted therapies. The global PSQI score in this investigation dropped dramatically from a mean of 8.4 to 6.0, which is noteworthy and may have therapeutic significance. Furthermore, after the therapy, the sleep efficiency scores rose from 82% to 89%, with 85% being the threshold for insomnia. As a result, the noted enhancement of this crucial menopausal symptom had a clinically noteworthy impact [8]. This study supports our findings since hot flushes cause an imbalance in the brain’s thermoregulatory centre, which makes people more likely to wake up during the night. By bringing hormone levels back to normal, yoga therapy helps to correct this imbalance and enhances the quality of sleep.
In contrast, Elavsky and McAuley’s [9] research states that physical activity, such as walking, has a beneficial effect on helping perimenopausal females achieve better sleep. It was a 4-month study where yoga was performed 2 times weekly for 4 months. For a duration of four months, the walking group was instructed to walk for an hour, three times a week. The Pittsburgh Sleep Quality Index was used to evaluate the nature of the participants’ slumber. The inter-group analysis of the Pittsburgh Sleep Quality Index did not differ significantly, but in the within-groups analysis, the walking group had a statistically noteworthy variation in improving the quality of sleep over the yoga group in perimenopausal females [9]. This research contradicts our findings, in which the treadmill group’s sleep quality differed significantly from that of the yoga group. Our six-week trial was too brief for the participants to reduce their weight and, as a result, improve their quality of sleep by lowering vasomotor symptoms.
Afonso et al. [10] conducted research on the efficacy of yoga in decreasing the symptoms of insomnia in menopausal females. The treatment duration for the yoga group lasted for 1 hour, 2 times per week for 4 months. The findings showed that, in comparison to the other groups, a substantial statistical difference was observed in the yoga group in post-treatment Insomnia Severity Index ratings. The authors claim that yoga has a neurophysiological basis for treating stress, anxiety, depression, and sleep issues. Prolactin and oxytocin secretion increase along with the autonomic tone and stress response systems, chemosensitivity decreases, the barore-flex response becomes more sensitive, and stimulation of the vagus nerve activates the parasympathetic nervous system. All these changes take place with regard to sleep parameters [10]. This research validates our findings because the sleep-wake cycle is caused by the hormone melatonin, which is only produced when a person is asleep. Because vasomotor symptoms interfere with sleep, perimenopausal females lack this hormone. Yoga promotes mental relaxation, which enhances melatonin hormone production and supports the circadian rhythm, both of which contribute to better sleep quality.
Cohen et al. [11] carried out a study to determine whether restorative yoga treatment for menopausal symptoms is feasible and acceptable. It was an 8-week study where yoga therapy for performed once weekly for 90 min, and the participants were asked to practice at home on the other days. Along with other outcome measures for various symptoms, the quality of the sleep was evaluated using the Insomnia Severity Index. The study’s findings indicated that the scores of the Insomnia Severity Index were statistically significant, thus improving the quality of sleep by restorative yoga therapy. This study is comparable to ours in that it found a connection between hot flashes and sleep disruptions. An imbalance in the brain’s thermoregulatory centre causes hot flushes. Better sleep quality results from overcoming this imbalance with the aid of yoga therapy [11].
Susanti et al. [12] conducted a randomised controlled trial on the impact of yoga therapy on females going through menopause and the quality of their sleep. Menopause’s overall effects on females going through menopause were assessed utilising the Menopause Rating Scale. According to this 20-week study, there was a substantial difference in the pre-post Menopause Rating Scale ratings among the females in the yoga treatment group. Yoga therapy helps to normalise the thermoregulatory centre in the brain, which is responsible for hot flushes [12]. Since there is a direct correlation between the quality of sleep and life satisfaction, this research lends validity to our findings. Vasomotor symptoms that interfere with sleep may cause a person to wake up frequently at night, which can impair their quality of life by making them feel exhausted and unproductive. By addressing these vasomotor symptoms, yoga therapy enhances the standard of living.
In India, Nayak et al. [13] studied how yoga treatment affected perimenopausal females’ physical and psychological quality of life. The Menopause-Specific Quality of Life Questionnaire was used to evaluate the standard of living of 216 perimenopausal females before and after the intervention. The trial lasted 12 weeks, and the intervention was practiced each day for 45 min. The intensive stretching and muscular training required to achieve and maintain yoga poses results in an increase in the oxidative potential of skeletal muscle and a decrease in glycogen consumption. Increased mitochondria, higher intramuscular oxygen and glycogen reserves, or greater vascularisation could all contribute to these outcomes.
The reason yoga seems to have this impact is that it modifies the neurological system, which modifies the alpha rhythm, brain homogeneity and intra-hemispheric coherence, and P 300 phase amplitude, all of which seem to be associated with improved cognitive function. Yoga treatment showed a considerable improvement over physical activity in the management of menopausal anxiety, a condition that can be extremely challenging to control. A variety of variables, including modified neurotransmitters, changes in cerebral blood flow, metabolism, and sympathetic activity, seem to be the cause for the improvement brought about by yoga practice [13]. This research backs up our findings because yoga treatment helps to increase joint proprioception, lengthen muscles, and lessen the aches and pains that lower a person’s overall quality of life.
Limitations
The limitations of this study were that no follow-up was undertaken after the 6 weeks of treatment, and the quality of sleep was not measured objectively, such as with the use of sleep monitors. Finally, we suggest that in order to gain a better understanding of the intervention’s effects, additional research can be conducted using diagnostic tools to measure levels of FSH and oestradiol before and after the intervention. Future researchers should consider using sleep monitoring devices and also extend the length of the study to improve the understanding of sleep disorders and improve prognoses.