Introduction
After a stroke, symptoms such as sensory-motor paralysis, spasticity and cognitive and perceptual disorders cause serious body asymmetry and unstable posture, leading to a decline in balance [1]. These symptoms hinder natural transitions in the gait cycle, including weight acceptance during the stance phase, weight transfer from the affected side to the unaffected side, and one-leg stance, which consequently alters the temporal and spatial parameters of walking [2]. In particular, walking speed and stance phase time of the unaffected side have a strong correlation with balance function in patients with post-stroke hemiparesis [3]. After a stroke, walking problems are characterised by slow speed, decreased cadence and stride length and asymmetrical weight distribution during double-limb support [4]. Although patients attempt compensatory movements on the unaffected side to maintain independence in daily life, these movements instead increase the risk of falls and hinder efficient walking. Therefore, the recovery of balance and walking functions is a major goal in stroke rehabilitation, which is essential for improving the quality of life and facilitating societal reintegration of patients after a stroke [5].
Based on the need for repetitive task training, treadmill training has been commonly used as walking training to simulate overground conditions in an indoor setting, which can be realised in a safe and easy way with a therapist’s guidance and speed control adjustments depending on the patient’s ability [6, 7]. indeed, treadmill walking entails the forwards transfer of lower limbs on moving belts, unlike walking on the ground, which requires active engagement of limb movement. Given that walking is a meaningful and familiar everyday task, treadmill training contributes to adaptation, achieved by emphasising functional tasks and active participation in the implementation of these tasks [8]. Also, repeated limb motions from treadmill training encourage symmetrical walking patterns, reduce hypertonia and improve cardiovascular-metabolic capacity during walking [9], which is helpful in improving the speed, distance and quality of walking [6]. in general, clinicians have highlighted the use of treadmill training as a means of restoring the decline in fitness levels caused by paralysis and abnormal energy consumption after a stroke. For this reason, the use of treadmill training is reasonable for clinical use in post-stroke patients [10].
Treadmill training is known to be more effective when the speed used is close to that of the age-matched normal population, which suggests an overload effect of the training [11, 12]. Walking training at a fast speed helps to negotiate challenging walking tasks in the community, such as irregular terrain, stairs, crosswalks and crowded roads. This suggests that the effects of treadmill training may improve when performed at the highest intensity possible within a tolerable range of cardiovascular fitness. However, high training speeds can impose significant physical strain on patients with lower fitness levels after a stroke. This implies that an individualised intervention is needed as a potential strategy for enhancing the abilities necessary to drive these patients’ ongoing recovery. This drive is beneficial in facilitating long-term participation in health-promoting physical activities [13]. Therefore, a performance-based approach that prudently adjusts training intensity based on patients’ comfortable walking speed is necessary to ensure safety and efficiency during treadmill training [14]. This indicates that they undergo performance-based treadmill training at a speed 1.3 times faster than their comfortable walking speed, as suggested by a previous study [15].
However, in clinical practice, self-selected speed during treadmill training has often been used to assess compliance and progress of patients with post-stroke hemiparesis [16]. This approach is considered insufficient for optimising the effects of treadmill training due to the relatively slow speed. despite the evidence supporting the benefits of treadmill training in the post-stroke population [7, 8], limited attention has been given to its impact on walking speed. Furthermore, previous studies employed cardiovascular monitoring to determine speed load during treadmill training [10–12, 17]; however, this can be challenging for clinicians with limited medical resources. To the best of our knowledge, despite the enhanced effects of treadmill training at higher loads, no previous studies have established standards for training speed in patients with chronic stroke [16, 18]. This limitation hinders the availability of evidence on the effects of high-intensity treadmill training tailored to individual walking ability. Therefore, the purpose of this study was to evaluate whether performance-based high-intensity treadmill training improves balance and walking function in patients with post-stroke hemiparesis. We hypothesised that participants who received performance-based high-intensity treadmill training, which included training at a higher speed tailored to their walking ability, would show more improvement in balance and walking function than participants who performed treadmill training at a self-adopted comfortable pace.
Subjects and methods
Participants
Twenty patients with post-stroke hemiparesis were recruited from two hospitals that provided inpatient rehabilitation services. Their diagnoses were made by physicians specialising in physical medicine and rehabilitation, each with over five years of experience. The participants were allocated into the experimental group (EG; n1 = 10) or control group (CG; n2 = 10) according to locational convenience. The criteria for selection were as follows: (1) > 6 months since stroke (disease codes in the iCd-11: 8B00 for intracerebral haemorrhage and 8B11 for cerebral ischaemic stroke) [19], (2) ability to independently walk with a time taken to cover 10 m in < 60 s (functional ambulation category: 3) [10], (3) no orthopaedic, cardiopulmonary or other neurological disorders that would influence treadmill walking and (4) no cognitive impairment ( 24 points in the Mini-Mental State Examination, MMSE) [20]. The patients were found to have a stable cardiovascular condition, albeit with a slightly higher risk for engaging in vigorous exercise compared to apparently healthy individuals (American Heart Association class B, toleration for aerobic capacity < 6 metabolic equivalents) [21]. Before the start of the experimental process, all the participants were provided with information about the procedure and safety of the study and signed a written informed consent.
Study design
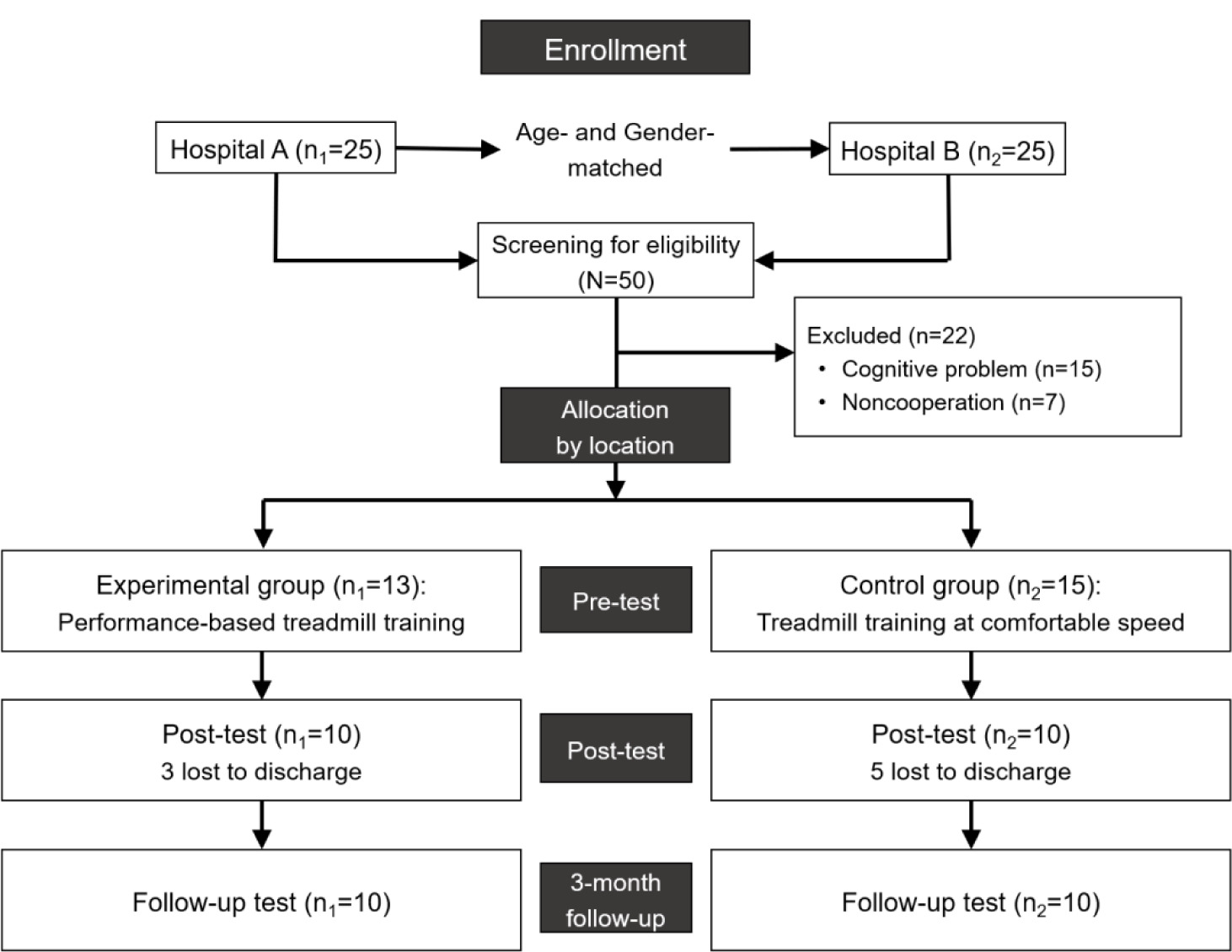
This study was a group-matched, single-blind preliminary trial. The participants were recruited from two hospitals in our region that were involved in our research programme. These hospitals were specialised rehabilitation centres for strokes located in a major city. one hospital was designated as the EG, in which the participants performed performance-based high-intensity treadmill training. The EG consisted of 10 participants who met the inclusion criteria. Ten age- and gender-matched participants were recruited from another hospital for the CG, and they performed treadmill training at self-adopted speeds. None of the participants were aware of their group allocation, and the person who conducted the assessment and data analysis was blinded to the study procedure and purpose. initially, 50 patients with post-stroke hemiparesis were recruited from two hospitals, 25 in each hospital. Thirteen participants in the EG and 15 participants in the CG, excluding 22 (12 in EG and 10 in CG) who were not eligible for selection, participated in the interventions. during the experimental process, 8 participants (3 in EG and 5 in CG) dropped out by discharge; consequently, data from 20 participants (10 in each group) were included in the final analysis (Figure 1). Based on the results of a previous study investigating the influence of speed in treadmill training [16], the power analysis (power of the study, 1 − = 85%; effect size, d = 1.17; significance level, < 0.05) suggested a sample size of 24 participants, 12 in each group. Although our sample size initially met the requirement calculated from the findings of previous studies, the number of dropouts remained a limitation in clearly defining our results, suggesting the need to recalculate the sample size based on the results of this study.
Outcome measures
10-metre walk test (10MWT)
The 10MWT was performed to measure walking speed. While the participants walked a straight route of 14 m at a comfortable speed, the time taken to cover the middle 10-m distance, excluding the 2 m at the start and end of the route, was measured using a stopwatch (iPhone, Apple, USA). The walking speed was then calculated. data from the 3 trials were averaged. The 10MWT has been reported to be highly reliable for clinical use in stroke (interclass Correlation Coefficient = 0.94) [22].
6-minute walk test (6MWT)
The 6MWT was performed on a 20-m straight route. Bars were placed at the start and end of the route, and then the participants were instructed to repeatedly shuttle between the bars for 6 min. The total distance the participants walked in 6 min was recorded in metres. The 6MWT has high test-re-test reliability in the post-stroke population [23].
Berg Balance Scale (BBS)
The BBS has been widely used to evaluate the balance ability of patients with stroke and is suitable for demonstrating these patients’ ability to maintain dynamic balance while carrying out functional tasks. The BBS consists of 14 items, each rated on a 5-point scale (0–4 points), with a total score of 56. The higher the score, the better the balance function. The BBS has been recognised to have excellent reliability and validity for the clinical assessment of balance and functional mobility in patients with stroke [24].
Activities-Specific Balance Confidence Scale (ABC)
The Korean version of the ABC scale is a self-administered tool to assess the balance confidence of patients with stroke. The ABC scale consists of 16 items to measure balance confidence related to specific daily activities. Scores are rated from 0% (not at all confident) to 100% (completely confident) for each item, with higher scores indicating higher balance confidence. The ABC has been reported to have high test-retest reliability (Cronbach’s alpha = 0.99) and validity [25].
Procedures
All the participants performed mat exercises, functional training and therapist-guided activities in a daily rehabilitation schedule. in addition, all the participants performed treadmill training with different speed options depending on the group after daily treatment. For the participants in the EG, the performance-based high-intensity treadmill training involved walking on a treadmill (WNT-2000T, Wellness Track, Gyunggi-do, Korea) at the maximum speed calculated based on the subject’s walking ability measured using the 10MWT (comfortable walking speed × 1.3) [15]. The participants’ comfortable walking speed was measured to determine the training speed before the intervention. For the participants in the CG, tread-mill training (Treksta-6000, Jeilfitness, incheon, Republic of Korea) was performed at a self-selected walking speed.
The treadmill training was performed for 30 min per session, twice per day, for 5 days over 2 weeks (a total of 20 sessions). To ensure the participants’ safety and prevent falls, a physical therapist was positioned behind them to provide immediate support for walking motion if needed. The walking speed was adjusted to the participants’ comfort level when they requested it, when walking instability was observed (such as backwards drift without immediate recovery and frequent toe dragging in mid-swing) and when there was a judgement of any safety risk during treadmill training. To compare the effects of treadmill training at different speeds in each group, measurements were performed at pre-test, post-test and 3-month follow-up.
Statistical analysis
The statistical analysis of all the data was performed using SPSS version 22.0 (Statistical Package for the Social Sciences, Chicago, USA). For the general characteristics of the subjects, homogeneity was tested using the chi-square and independent t-tests. Between-group comparisons were analysed using independent t-tests. Within-group comparisons were analysed using one-way repeated-measures analysis of variance, and a post hoc test with Bonferroni adjustment was used for multiple pairwise comparisons when significant differences were found. The statistical significance level was set at p < 0.05.
Results
General characteristics of the subjects
The general characteristics of the participants are presented in Table 1. Gender, age, height, weight, MMSE-K scores, stroke type and onset duration were not significantly different between the groups (p > 0.05).
Table 1
General characteristics of participants in the two study groups
Comparison of data collected at pre- and post-test and 3-month follow-up between the two groups
Table 2 summarises the results of the comparison of data across measurement times between the groups. in the between-group comparison, no significant differences were found in any of the parameters at pre-test (10MWT: t = –0.71 and p = 0.49; 6MWT: t = –0.94 and p = 0.36; BBS: t = –1.39 and p = 0.18; ABC: t = –0.69 and p = 0.50), post-test (10MWT: t = 0.47 and p = 0.65; 6MWT: t = –0.13 and p = 0.90; BBS: t = –0.42 and p = 0.68; ABC: t = 0.59 and p = 0.57) or at the 3-month follow-up (10MWT: t = 1.37 and p = 0.19; 6MWT: t = 1.40 and p = 0.18; BBS: t = –0.33 and p = 0.75; ABC: t = 0.47 and p = 0.65). However, significant differences (p < 0.05) were observed in the change values for the 10MWT and 6MWT between pre- and post-test, as well as between pre-test and 3-month follow-up. Additionally, significant differences were found in the change values for the BBS and ABC scores between pre- and post-test. in these parameters, effect sizes (d) were mostly maintained above 0.8, indicating a large effect related to the intervention [26].
Table 2
Between-group comparison of each variable across the measurement times
Furthermore, in the within-group comparison, subjects in the EG showed significant differences in 10MWT (F = 6.68, p = 0.02), 6MWT (F = 7.20, p = 0.02), BBS (F = 5.75, p = 0.03) and ABC (F = 5.58, p = 0.03) scores across the measurement times. The post hoc test results showed that the 10MWT and 6MWT values were significantly different between preand post-test and between pre-test and 3-month follow-up. The BBS and ABC scores showed significant differences between pre-test and 3-month follow-up, respectively. However, in the CG, a significant difference in the ABC score was found (F = 7.00, p = 0.02), with post hoc test results showing a significant difference between pre- and post-test.
Discussion
This study supports the idea that performance-based high-intensity treadmill training may be favourably used to improve the balance and walking functions of patients with post-stroke hemiparesis.
In general, clinical observation has shown that fast-speed treadmill training offers some advantages in restoring walking function after stroke [10, 15, 27]. despite its benefits, in clinical practice, the speed load of training is often determined according to patient and/or therapist convenience without clear guidelines [28]. Lee [16] suggested employing a walking speed of 1.2–1.3 m/s during training, which exceeds the average walking speed of patients with chronic stroke. However, a higher training load can impose a heavy burden on the physical and emotional well-being of slow walkers with low fitness levels. This suggests that the training load should be individualised based on the walking capability of patients with post-stroke hemiparesis to optimise training effects.
While previous studies supported the use of heart rate for determining walking speed during treadmill training [29, 30], many factors can influence heart rate, making it often an inappropriate approach for determining walking speed in patients with post-stroke hemiparesis. Furthermore, although cardiovascular monitoring can efficiently regulate training intensity, there is a need for an alternative approach for clinicians who lack access to this procedure. Based on this concept, this study employed performance-based high-intensity treadmill training, tailored to the participants’ walking abilities, as the primary intervention. As supported by a previous study [15], the training speed in this study was set at 1.3 times the comfortable walking speed of each participant, a method that could be easily adopted in a clinical setting.
In this study, participants in the EG demonstrated greater improvement in their 10MWT scores after the intervention compared to those in the CG, and these gains were maintained at a 3-month follow-up. A possible explanation for these findings is that those in the EG were primarily trained for walking performance, resulting in positive changes in neuromuscular control during repeated limb motions. Research involving healthy individuals suggests that high-speed training increases neural input to the muscles during rapid dynamic actions [31]. The overall elevation in motor neuron excitation could be due to increased excitatory input, reduced inhibitory input or a combination of both. Hence, for patients with chronic stroke, engaging in high-speed treadmill training could potentially induce changes in neurophysiological mechanisms, leading to increased neural input to the lower limbs and enhancing motor neuron excitation.
Moreover, treadmill training at fast speeds offers a greater opportunity to promote locomotor control through intensive practice of walking movements [17, 32]. Changes in the lower limbs resulting from such training could potentially lead to positive changes in gait parameters and performance, which correlate with more symmetrical patterns of limb use during walking. in addition, the restoration of walking velocity has been identified as one of the most crucial indicators of functional status and clinical improvement in patients with post-stroke hemiparesis [33]. Walking velocity strongly correlates with walking independence, which is a significant factor in determining functional independence [34]. Therefore, performance-based high-intensity treadmill training, as described in this study, may be beneficial for enhancing functional mobility recovery.
In this study, the improvements in the 6MWT and BBS scores in the EG after the intervention were > 40 m and > 3.50 points, respectively, which met the criteria for the minimum detectable change (6MWT: 36.6 m and BBS: 2.7 points) [32, 34]. The BBS includes various items that are important for walking. Although the individual item scores of the BBS were not presented in detail in this study, the total score – which is the sum of the scores of all items – indicates that the patient can safely perform a series of tasks related to sitting, standing and dynamic balance [35].
Furthermore, a recent study has reported that walking speed may be closely related to balance function after stroke [3, 36]. Therefore, improvement in BBS scores is thought to be related to the improvement in the 10MWT and 6MWT values [37]. These results align with those of previous studies investigating the effects of treadmill training at fast speeds [17, 18, 38]. This implies that our method, which sets the speed load for high-intensity treadmill training based on individual walking capability, may be a useful and easily accessible approach in clinical settings because it does not require any devices or complicated procedures. Balance and walking abilities are key indicators of functional recovery and activity independence after stroke [36]. Therefore, in this study, improved balance and walking function suggest that performance-based high-intensity treadmill training is clinically feasible and may enable individuals to return to daily activities after stroke.
Patients with post-stroke hemiparesis often have lower tolerance for sustained movements due to decreased aerobic fitness levels, a major factor contributing to inactive lifestyles [27]. Therefore, effective solutions need to be developed to enhance the training effects in stroke rehabilitation. Recent systematic reviews have supported the psychological benefits and cardiovascular advantages of treadmill training [38], contributing to the ability to perform overground walking and thereby facilitating rehabilitation effects [17]. Specifically, walking training at fast speeds highlights intensive, repetitive movements of the lower limbs with greater effort [39], which helps to improve fitness levels and facilitate alternating limb control after stroke. Therefore, the improved 6MWT value after the intervention may be one of the greatest benefits of the training, indicating positive effects on walking endurance. in this study, the 6MWT value improved by an average of 41.0 m in the EG, which exceeded the 34.4-m criterion for the minimal clinically important difference [40].
Walking endurance is closely related to self-efficacy and quality of life after stroke. Task self-efficacy may be the most common factor in maintaining a physically active lifestyle, reducing emotional stress and enhancing daily activities. A crucial role of a conditioning programme, including treadmill walking training, may be to promote physical fitness and skill competency among participants [41], with the potential to positively influence their lifestyles through improved self-efficacy. As observed in this study, despite no difference between the groups at the 3-month follow-up measurement, the improved ABC scores after the intervention indicate that performance-based high-intensity treadmill training may be more effective than training at self-adopted speeds in addressing psychological issues, such as balance confidence and fall efficacy.
This study has some limitations. First, the sample size was relatively small, limiting the generalisability of our findings to the broader stroke patient population. Based on the results of this study, power analysis (power of the study, 1 − = 85%; effect size, d = 1.30; significance level, < 0.05) revealed that 30 participants are necessary for a definitive conclusion, 15 in each group. Second, we only observed the training effects for 3 months after the intervention, making it difficult to assess the long-term effects. Third, this study focused on explaining the effects in clinical practice, which could not be fully captured by the quantitative data on walking. Finally, given our participants were recruited from two hospitals, it is important to note that potential effects stemming from variations in daily rehabilitation schedules and distinct characteristics between the hospitals cannot be ruled out. in addition, a significant bias in this study could arise if participants from one hospital always received treatment, while those from the other hospital did not. Therefore, further studies with more robust designs are necessary.
Conclusions
In stroke rehabilitation, the recovery of balance and walking functions is the most important goal for ensuring independence in daily life. Recent research has shown that treadmill training at fast speeds can help restore walking function. individual performance levels related to walking ability should be taken into consideration when determining the speed load during training, because this is crucial for ensuring both safety and efficiency. The purpose of this study was to assess the effectiveness of performance-based high-intensity treadmill training on balance and walking functions in patients with post-stroke hemiparesis. The findings suggest that treadmill training performed at a brisk pace, adjusted according to the patient’s comfortable speed, may be more effective in improving balance and walking than training at a self-selected pace. Therefore, greater benefits from treadmill training following a stroke may be achieved by setting higher, individualised speed loads tailored to each patient’s walking performance. Further research with a more robust design and longer-term follow-up will be necessary to explore this approach in greater depth.