Introduction
Acute lymphoblastic leukaemia (ALL) is a common type of childhood leukaemia and is a heterogeneous haematological disease [1]. It represents approximately 80% of acute leukaemia features over a wide variety of biological and clinical aspects [2], and includes the proliferation, accumulation and infiltration of lymphoid blasts that invade the bone marrow and reduce the production of blood cells, leading to anaemia, infections, and haemorrhage [3, 4].
Although many children and adolescents who are treated for cancer show improvements in balance defects after treatment, their results are still below those of normal subjects six months after treatment [5]. Chemotherapy can negatively impact the ability of the child to respond appropriately to changes in the centre of mass, and the processing of sensory information can be negatively impacted by chemotherapy [6].
Corticosteroids have detrimental effects on muscle flexibility and strength that are manifested as prolonged motor-evoked potential latencies [7] resulting in an elevated risk of obesity after cancer treatment, which in turn can exacerbate balance-related issues by limiting the child’s muscular force and range of motion [8]. Therefore, these children are more likely to have difficulties in balancing because of motor, muscular, potential somatosensory, and cognitive impairments [6].
The benefits of physiotherapy programs for a variety of childhood disabilities, including systems (skeletal, neuromuscular, and cardiovascular) and disturbances in postural balance, have been investigated. Physical therapy, either during or shortly after cancer treatment, can prevent or markedly reduce the severity of adverse effects. In addition, physiotherapy intervention is important in enhancing the quality of life of children as a result of a number of interventions introduced to lessen their vulnerability to disease. Static postural sway can be reduced, and dynamic balance can be enhanced through balance training [9].
Treadmill training involves proprioceptive feedback that improves functional performance and postural balance [10]. Treadmill training promotes the kinematic, kinetic, and temporal features of walking, improves motor learning, enhances functional abilities of the lower limbs and muscle strength, and activates the locomotor control system [11].
There is a lack of knowledge, and limited studies have focused on the impact of treadmill training on balance in children with ALL. Therefore, in the current study, we aimed to examine the impact of treadmill training on balance after six months of chemotherapy in children with ALL.
Subjects and methods
Design of the current study
This was a randomised controlled trial. All participating children provided their informed consent to participate. The study was conducted from July to December 2022.
Randomisation
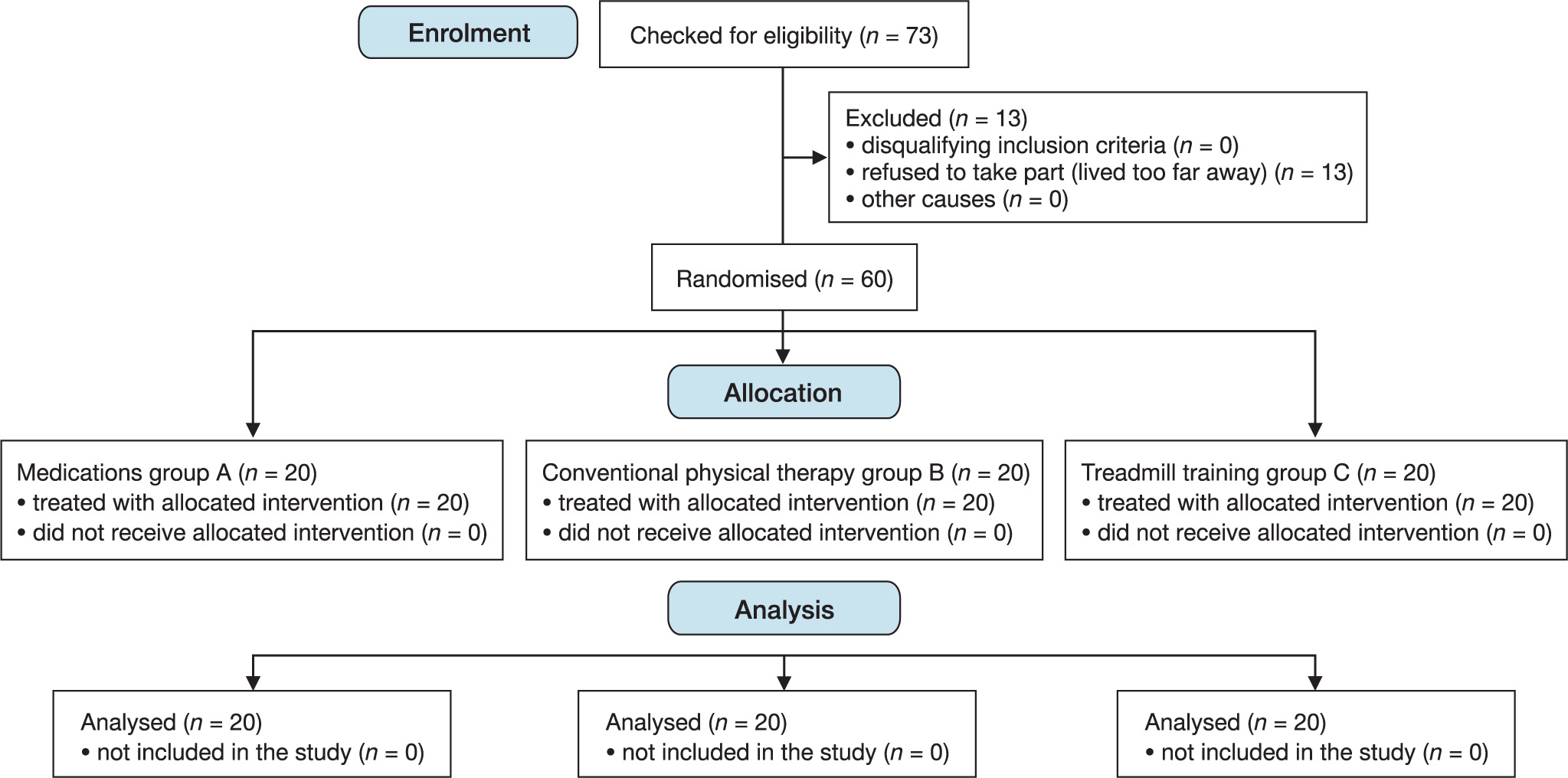
According to the flowchart in (Figure 1), 73 children met the inclusion criteria for the study; however, 13 dropped out because they lived too far away. Block-stratified randomisation software (Randexe, Windows version 6.0, block sizes 4, 8, 2, and 6) was used to randomly assign the remaining 60 children with ALL at a 1:1:1 allocation ratio. The concealed allocation was performed using sealed, sequentially numbered, opaque envelopes. Moreover, it was challenging to divide the samples into three equal groups with the same numbers in this randomised program because of the presence of multiple stratified variables [12]. Randomisation was performed by a blinded researcher who was not involved in the recruitment, data collection, or treatment.
Participants
Sixty children with ALL of both sexes were recruited from the Abou El-Rish Hospital and the National Cancer Institute’s outpatient clinic in Cairo and were then recruited at the out-patient clinics of the Faculty of Physical Therapy, Modern University for Technology and Information, Cairo, Egypt.
The inclusion criteria were as follows: (1) children with ALL who had completed six months of chemotherapy [13], (2) children aged 8–12 years, (3) medically stable; (4) mentally capable of participating in the study; and (5) those who could stand and walk without constant assistance or falling repeatedly. Children with psychological or neurological (impairment of sensation) problems, musculoskeletal (fixed deformity or tightness in the lower limbs) problems, limitations in mobility, heart abnormalities, or impaired hearing or vision were excluded.
The participants were divided into 3 groups of equal size. All the participants in the three groups were provided with the recommended standard medical care. Group A received medical treatment, group B received a conventional physical therapy program and medical treatment, and group C was treated with treadmill training and medical treatment.
Measurements used
The total time required for the assessment was approximately 40 min for each child and the evaluation was applied pre and post the eight weeks of the training program. All procedures were explained to the participating children before starting the evaluation. The assessment sheet, including the variables evaluated pre and post treatment program, was maintained for each child who participated in this study.
Balance Master System (BMS) (NeuroCom Smart Balance Master)
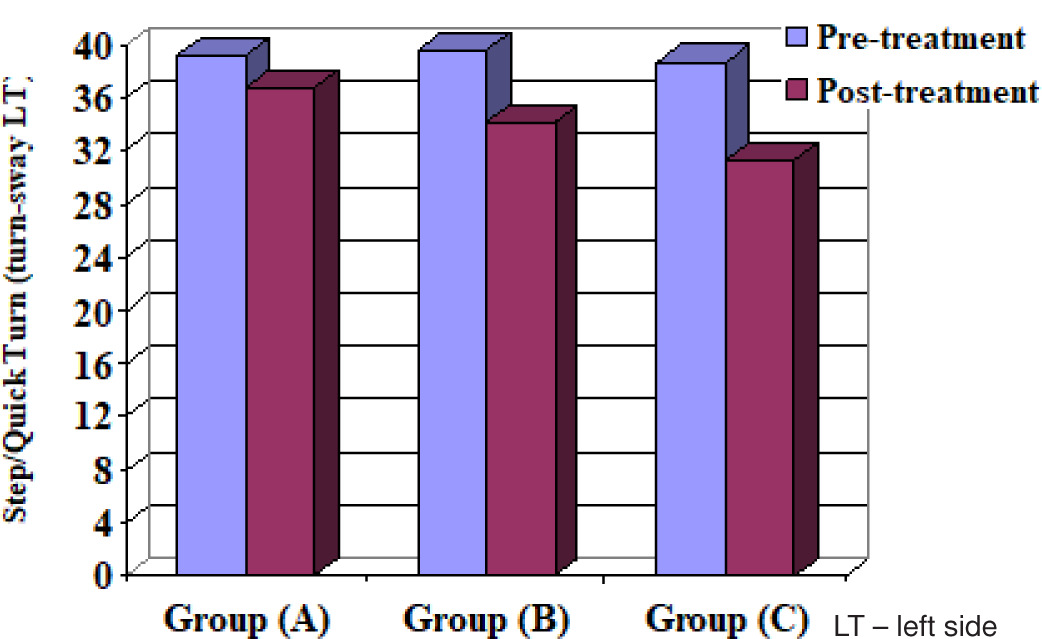
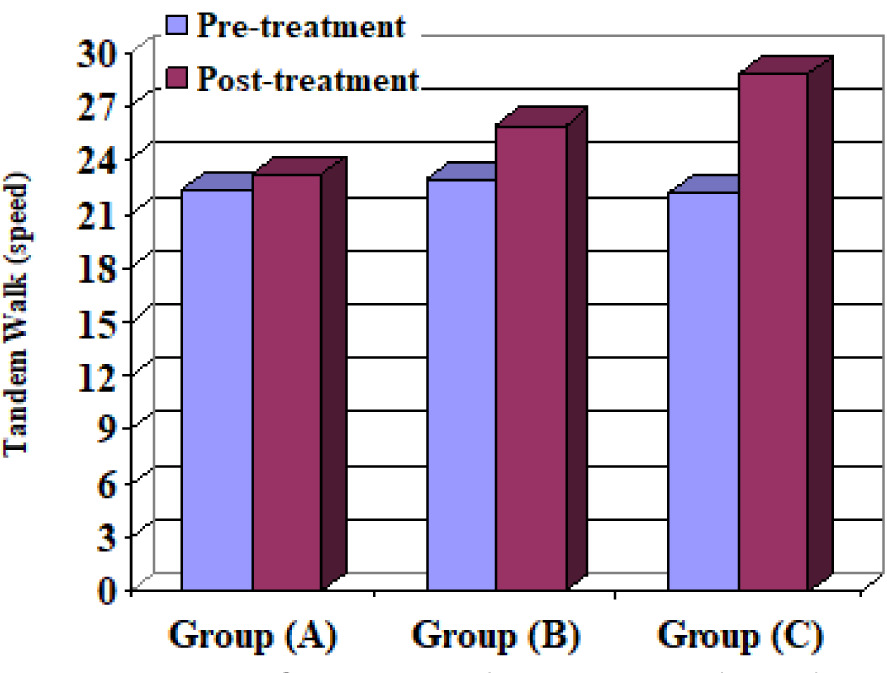
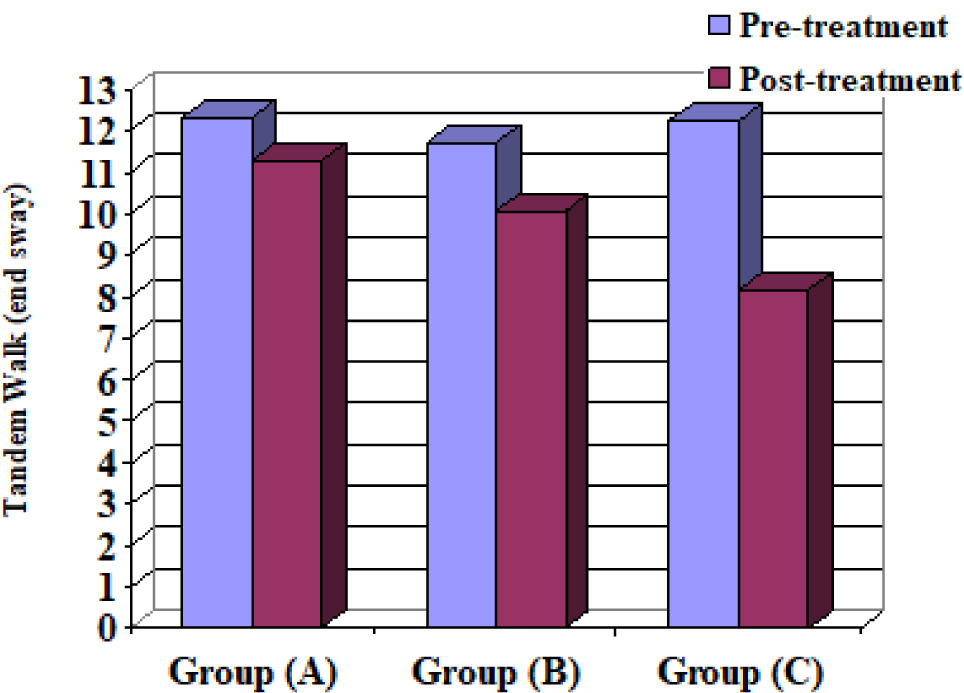
This is the most reliable test for measuring balance and has valid values for functional balance performance [14]. Postural sway measures, reactive strategies, sensory strategies, and proactive balance control can all be identified and quantified using this computerised system [15]. It is a reliable and objective tool for assessing balance and postural control [16]. The BMS has a screen, two force platforms, and a computer main body. The participating children stood at the centre of the two plates after taking off their shoes. The children folded their arms and looked at the monitor in front of them [17]. The following BMS tests were used to assess the three groups: Step/Quick Turn (turn-time RT and LT) (turn-sway RT and LT) and Tandem Walk (speed and end sway).
Biodex Balance System (BBS) (Biodex Medical Systems, Version 3.1)
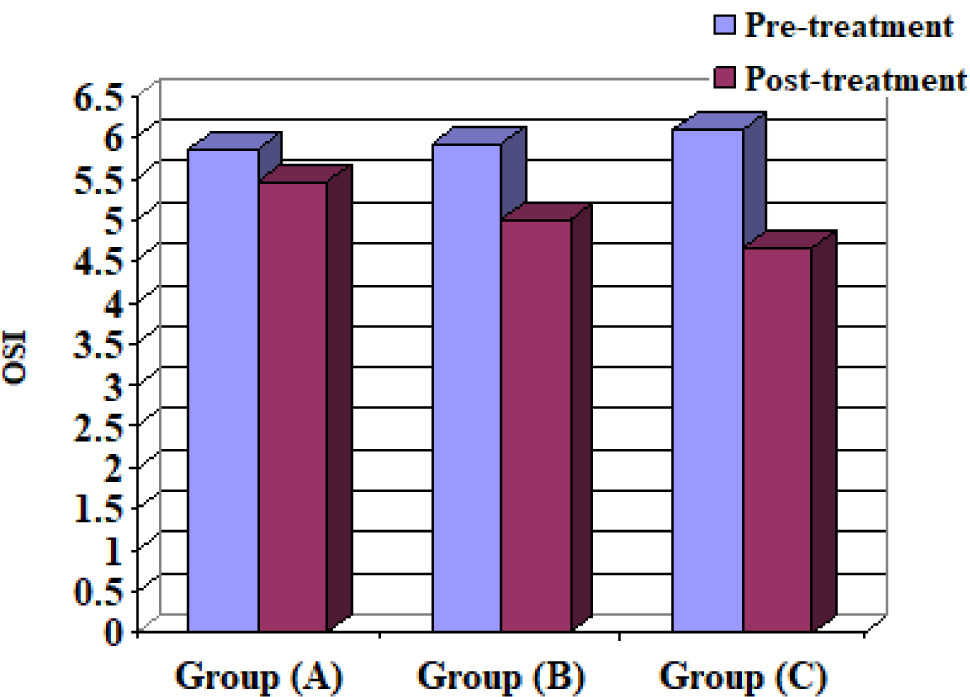
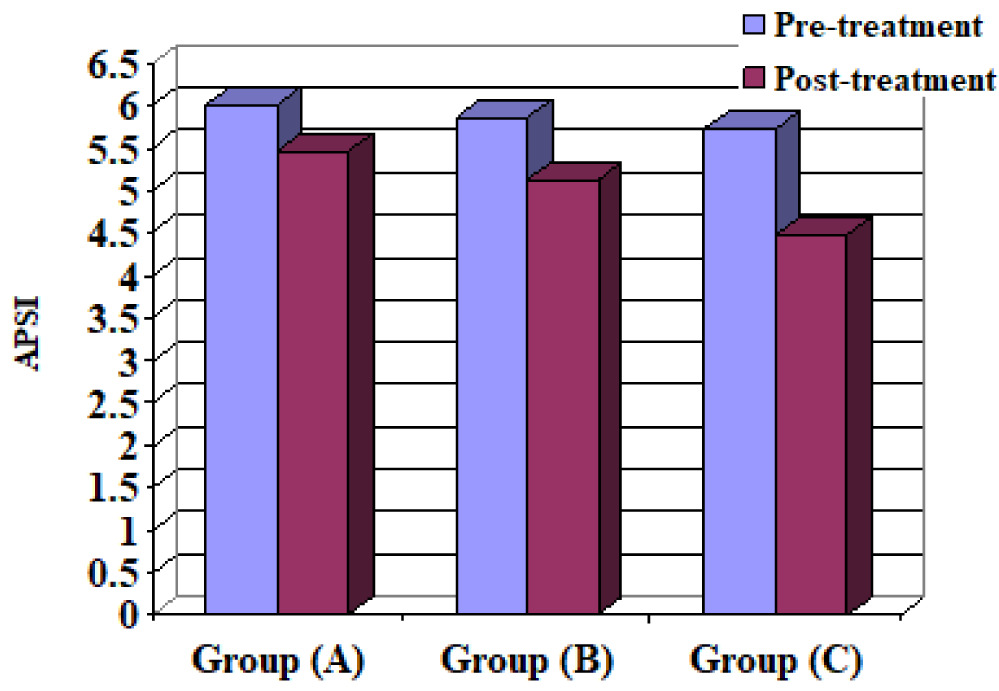
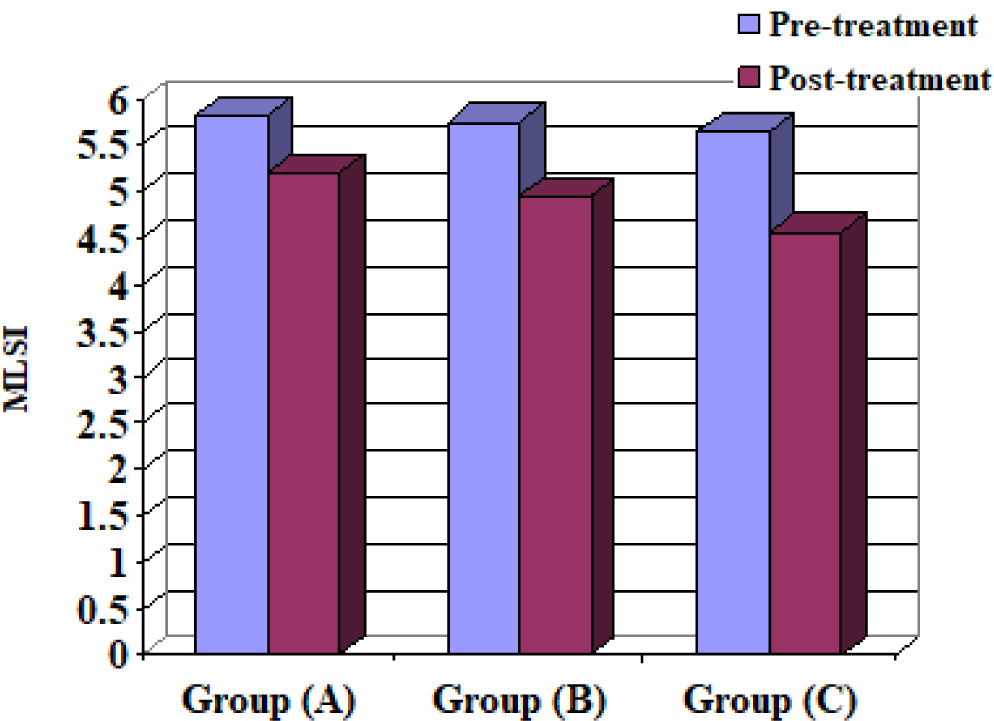
It is a reliable and objective assessment tool for quantifying dynamic balance, and the reliability indices of the overall stability index (OSI), anteroposterior stability index (APSI), and mediolateral stability index (MLSI) are 0.43, 0.80, and 0.82, respectively [18,19]. This technique is used to adjust the stability of a suspended circular force plate. The force platform can be tilted up to a maximum of 200° in any direction and measures the participant’s balance by how far the platform moves away from its centre [20]. The BBS assesses neuro-muscular control by stimulating the joint mechanoreceptors and maintaining dynamic postural stability [19]. The OSI, APSI, and MLSI were evaluated in this study.
Intervention
In group B, the conventional physical therapy program was applied for 60 min; 8 weeks of the treatment program was applied for 3 sessions per week. Vestibular boards, blocks, rolls, and wedges of varying sizes were used in the conventional physical therapy to enhance and control balance posture (Table 1) [21].
Table 1
Treatment program utilised for group B
In group C, the participants received 30 min of treadmill training and were instructed to take steps on a motorised treadmill (ENTRED, Enraf-Nonius) at approximately 75% of overground speed for 20 min, while walking independently at a 0% incline. Before beginning their treadmill workout, each child spent five minutes warming up by performing stretching exercises (20–30 s per stretch, 3–5 times for each muscle) of the quadriceps, Achilles tendon, and hamstrings [22].
The therapist adjusted the hand rail height on the tread-mill so that the children could stand correctly while using the machine. To promote free walking, it should be noted that the child should keep looking forward while walking on a treadmill. When the child completed three stages of 1-minute training cycles on the treadmill, the training was considered complete. In the first stage, the child used both hands to hold onto the rails for the first 15 s of every minute. In the second stage, in the subsequent 15 s, the child started holding onto the railings with one hand. In the final stage, the child did not hold onto the railings for the last 30 s. This procedure was repeated 20 times for each child [23]. There was a 5-minute cool-down, including stretching exercises, at the end of the program to prevent any spasms from developing. During the program, each child wore stretchy clothes and shoes that did not hurt their feet [24].
Statistical analysis
Sex distribution was tested using the chi-square test. Means and standard deviations were used to summarise the data. The Shapiro–Wilk test was used to verify that the data followed a normal distribution. Levene’s test was applied to examine whether there was homogeneity of variance across groups. Analysis of variance (ANOVA), multivariate analysis (3 × 2) of variance (MANOVA), and the Bonferroni correction (post-hoc) test were used to assess whether the three groups differed significantly from one another. In this study, we considered a result to be statistically significant if it had a p-value of 0.05. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 22 for Windows (IBM SPSS, Chicago, IL, USA). The F-test MANOVA within and between interaction effects was performed using the G*POWER statistical software (version 3.1.9.2; Franz Faul, Universitat Kiel, Germany). Considering = 0.05, G*Power = 80% and effect size = 0.73, a minimum of 20 subjects per group and a maximum of 60 subjects were needed to generate a valid sample size.
Results
Children’s demographic data
There were no substantial differences among groups A, B, and C in mean age (p > 0.05) (Table 2).
Sex distribution
There were no significant differences between the 3 groups A, B, and C (p > 0.05) (Table 3).
Measurements Before treatment for groups A, B and C
When comparing the pre-treatment mean ± SD values, non-significant differences of all measurable variables were revealed between the 3 groups (p > 0.05) (Table 4).
Table 4
Step/Quick Turn (turn-time RT and LT) and (turn-sway RT and LT), Tandem Walk (speed and end sway), OSI, APSI and MLSI for the 3 groups A, B and C
Before and after treatment for groups A, B and C
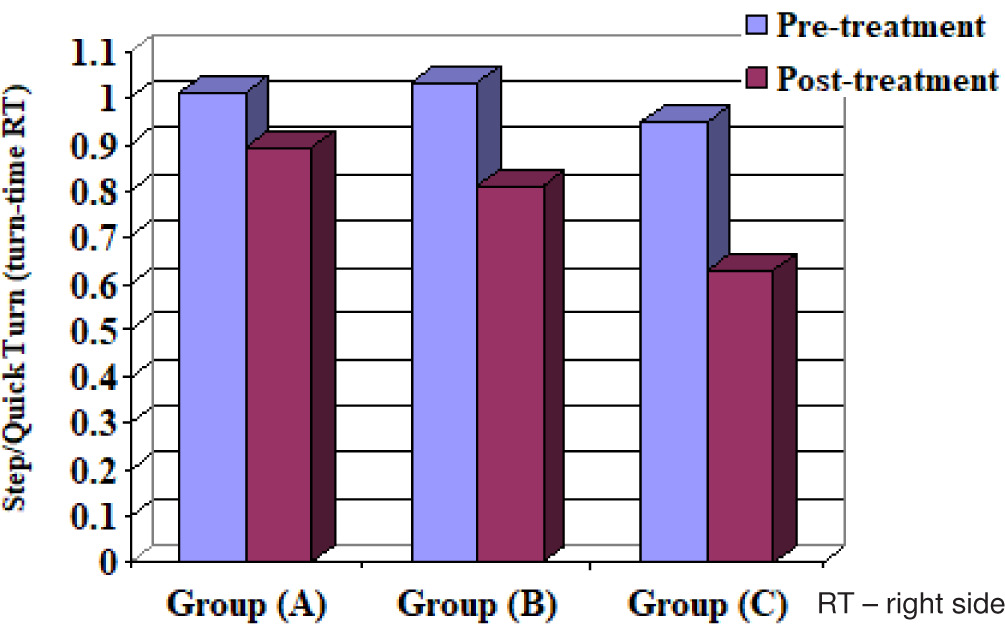
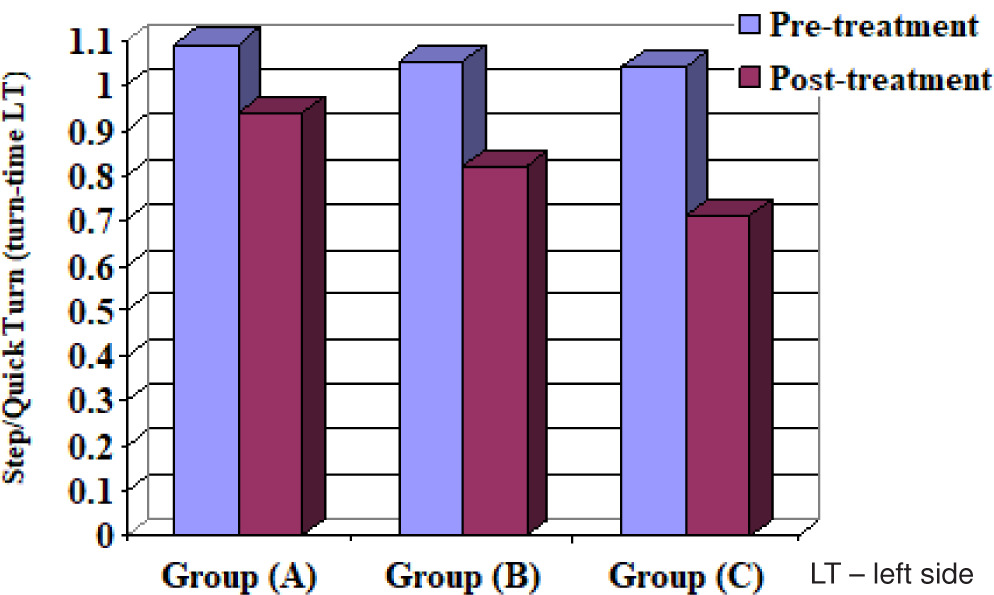
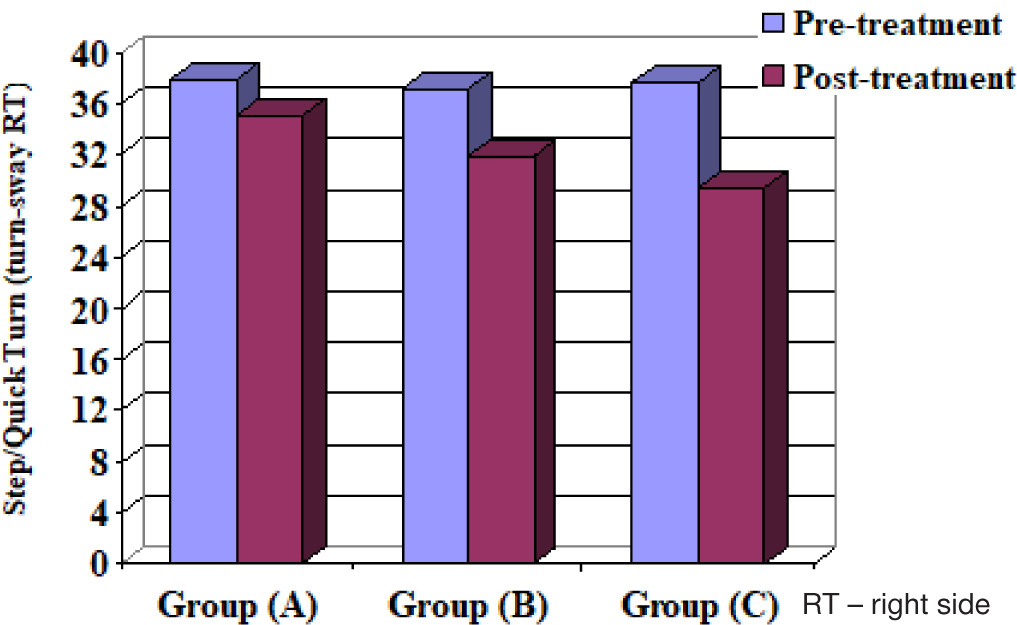
When comparing the pre- and post-treatment mean ± SD values, significant differences for all measurable variables were revealed between the 3 groups (p < 0.05) (Table 4) (Figures 2–10).
After treatment comparisons between groups A, B and C
When comparing the post-treatment mean ± SD values, significant differences of all measurable variables were revealed between the 3 groups (p < 0.05) (Table 4).
After treatment between groups A and B, groups A and C, and groups B and C
When comparing the post-treatment mean ± SD values among groups A and B, A and C as well as B and C, all measurable variables showed significant differences between the 2 groups (p < 0.05) (Table 5, Figures 2–10).
Table 5
After treatment of Step/Quick Turn (turn-time RT and LT) and (turn-sway RT and LT), Tandem Walk (speed and end sway), OSI, APSI and MLSI between groups A and B, groups A and C, and groups B and C
Discussion
The current study investigated the impact of treadmill training on balance in children with ALL after six months of chemotherapy. We observed significant differences in all measurable variables before and after treatment among the 3 groups. There was a significant difference in post-treatment mean values that favoured the treadmill group (group C) and the conventional physical therapy group (group B), and in favour of the treadmill group compared to the conventional physical therapy group.
The current study involved ALL, which is an important classification of leukaemia. This was confirmed by Park et al. [25], who noted that ALL was the most prevalent type of leukaemia in children. Tanir and Kuguoglu [26] agreed that children should be selected when they are between the ages of 8 and 12 and found that children’s balance performance began to resemble that of adults between 8 and 12 years.
Murat et al. [27] found that muscle weakness was a significant clinical sign in patients with ALL, even during maintenance of the ALL therapy phase. This current data are in agreement with the hypothesis that impairment of the muscle function may be an important sign in children with ALL, and we further extended this hypothesis to children 1 year after the end of malignancy treatment.
According to Varedi et al. [28], balance is a minor problem in people with cancer. A systematic review revealed that the impact of cancer on balance in children with ALL remains unclear. Some studies have shown that balance in patients was significantly affected, whereas others have found little to no effect on balance. Chemotherapy administered to children with ALL can affect balance, including reduced flexibility and muscle strength, and sensory and motor peripheral neuropathy. In this study, the balance performance of children with ALL was highly affected before initiating the treatment program, which may have resulted from direct infiltration by cancer cells, pressure from the tumour, fibrosis as a result of radiation therapy, neurotoxicity as a result of chemotherapy, or even paraneoplastic disorders [26].
However, studies of the effect of conventional physiotherapy programs on balance in children with ALL are limited. The results of our study in group B agree with a study by Zakaria et al. [13], which revealed that balance improvement among children with ALL after six months of chemotherapy resulted from balancing exercises and gait training therapy. Furthermore, Tanir and Kuguoglu [26] reported that children with ALL who implemented a systematic and regular program of physical therapy exercises showed improvements in their test scores, physical abilities, and laboratory results.
In addition, a comparison of the pre- and post-treatment results of group B are confirmed by Marchese et al. [29], who reported that two key bodily functions essential to normal gait were enhanced following physical therapy intervention for children with ALL receiving chemotherapy. Strength as well as quality of life may be enhanced by physical therapy programs that begin earlier in the course of treatment and place greater emphasis on endurance. Strength in ankle dorsiflexion and knee extension, two measures of balance, was found to increase after 4 months of intervention (strength and balance exercises) in children with ALL, lending credence to our findings.
Also, a comparison between the results of the pre-and post-treatment programs in the mean values of group C aligned with those found by Zakaria et al. [13], who found that gait training using a treadmill can help in strengthening the body’s musculature, enhancing posture, balance, endurance, and increasing body movements, leading to improved postural balance and decreasing the risk of falls. In addition, the post-treatment results of group C are in agreement with the findings of Rose et al. [30] and Grecco et al. [31], who demonstrated that treadmill training has significant effects on static and dynamic balance compared with overground gait training. After 12 sessions at the aerobic threshold, results were observed without body weight support. These findings indicate that improved functional performance and motor effects can lead to greater independence and improved balance.
Furthermore, from other studies supporting group C for enhancing balance and muscle strength, a study performed by Yeh et al. [32] supported our findings by reporting improvements in knee extension and ankle flexion strength in children with ALL after six weeks of supervised treadmill training.
Based on our results, the superior results of groups B and C were supported by the results of Bakya and Elhakk [33], who found that combining a 16-week aerobic treadmill program with physical therapy significantly increased children’s fitness and decreased their fatigue. Additionally, balance, stability, and coordination patterns can be improved by tread-mill training [34].
A comparison of the post-treatment results between groups B and C in favour of group C showed improvement in somatosensory function and coordination, which are two of the basic components of balance. Children with ALL may have difficulty integrating sensory information, which can affect their motor skills and balance after chemotherapy. Additionally, weaknesses or coordination issues can make maintaining balance more challenging. The children in group C in this study may have improved their somatosensory and coordination problems after treadmill training compared with those in group B because regular exercise on a treadmill may enhance the child’s ability to maintain balance by improving their sensory feedback and motor responses.
Treadmill exercises in group C may help integrate sensory information from the feet and legs, which is important for balance. Improved sensory feedback from regular exercise can potentially improve spatial awareness and motor responses. Treadmills are more effective in utilising and enhancing somatosensory inputs such as proprioception.
Limitations
The study’s limitations include the small sample size and the fact that the effects of the interventions were only evaluated after eight weeks.
Conclusions
Treadmill training is an efficient tool for enhancing balance in children with ALL after chemotherapy. The positive outcomes observed provide a foundation for further research exploring the long-term benefits of treatment and its potential to enhance the overall functional abilities in children.
As balance is crucial for daily activities, future interventions should focus on integrating treadmill training with comprehensive rehabilitation programs for children with ALL.