Introduction
In recent years, the rehabilitation system in Ukraine has been rapidly developing. The foundation for creating a modern rehabilitation system was established by the Law of Ukraine ‘On Rehabilitation in Healthcare’, adopted at the end of 2020 [1].
Prior to 2020, rehabilitation in Ukraine, including physiotherapy, underwent a complex and gradual process of development – from a generalised concept of physical rehabilitation to the establishment of distinct specialisations such as physiotherapy, occupational therapy, and speech and language therapy. Physiotherapy in Ukraine was undergoing a gradual transformation, with traditional approaches primarily focused on medical massage, therapeutic exercise, and basic functional restoration. The development of the rehabilitation field was significantly influenced by international models, particularly the Canadian and Polish schools of physiotherapy, which contributed to the integration of evidence-based practices and a more holistic understanding of patient-centred care.
Unfortunately, this significant advancement in rehabilitation was driven by the military conflict that began in 2014 and escalated in February 2022. The war has significantly increased the need for rehabilitation services for both injured military personnel and civilians [2].
The Ministry of Health of Ukraine is responsible for the development of the rehabilitation system, including its legal framework and workforce support. Efforts are focused on addressing modern challenges such as the insufficient number of qualified rehabilitation professionals [3], the need to train professionals in evidence-based practices [3–5], unequal access to rehabilitation services in rural and frontline areas [6], and the underdevelopment of patient routing systems [7], among others.
At the same time, the war has led to a dramatic rise in the number of patients, particularly those with severe injuries caused by mines, explosions, or firearms, requiring high-quality rehabilitation services [8]. This situation overwhelms all professionals in multidisciplinary teams, significantly increasing their risk of developing professional burnout (PB). These professionals work under challenging conditions, daily encountering emotionally taxing situations while rehabilitating patients who have suffered severe injuries, losses, or psychological trauma. This environment exacerbates emotional exhaustion, chronic fatigue, cynicism, and reduced productivity and work quality.
Unfortunately, there is limited research available on the impact of military conflicts on PB among healthcare workers, especially rehabilitation professionals. For instance, Adler et al. [9] examined factors influencing PB among military medical personnel in the U.S. Armed Forces during service in Afghanistan. They found that self-care, team support, and leadership were promising areas for reducing burnout among medical staff. Similarly, Sargent et al. [10] studied PB in a military medical centre during wartime, finding burnout levels similar to those observed in civilian medical centres. Research by Alhaffar et al. [11] focused on PB among physicians in Syria, revealing that 93.75% of doctors in the sample had high levels of burnout in at least one dimension, with 19.3% of residents exhibiting high levels across all three dimensions.
Some studies have explored PB among future or practicing rehabilitation professionals, examining various conditions and socio-demographic factors. However, these studies offer conflicting results regarding factors influencing PB development or existing links with burnout [12–19].
The aim of our study is to assess the degree of PB among Ukrainian rehabilitation professionals in the context of military conflict. We formulated the following research questions:
What is the level of PB across the dimensions of emotional exhaustion (EE), depersonalisation (DP), and professional accomplishment (PA) among Ukrainian rehabilitation professionals (physical therapists, occupational therapists, their assistants, and physicians in physical and rehabilitation medicine) in the context of military conflict?
Does the level of PB depend on unmodifiable factors such as sex, position, work experience, and the location of healthcare facilities relative to the front line?
What PB profiles are characteristic of rehabilitation professionals?
Answers to these questions will help in developing effective strategies and programs for preventing PB and supporting the physical and mental health of rehabilitation professionals.
Subjects and methods
This is a cross-sectional study of rehabilitation professionals in Ukraine. Participation was voluntary, and data were collected using a Google Forms questionnaire distributed via the social media platform Facebook. Personal data (name, surname, age, email) were not collected to prevent participant identification. The data were compiled into an Excel table, with access securely protected.
A total of 112 rehabilitation professionals working in multi-disciplinary teams participated in the study, including physical therapists, occupational therapists, their assistants, and physicians specialising in physical and rehabilitation medicine. Among them were 39 males and 73 females. The primary inclusion criterion was holding a rehabilitation specialist position in a healthcare facility. The participants included 67 physical therapists (PT), 12 occupational therapists (OT), 25 assistants (PT/OT), and 8 physicians in physical and rehabilitation medicine (PRM). The analysis considered work experience (less than 2 years, 2–5 years, 6–15 years, over 15 years) and the location of healthcare facilities (frontline and central-western regions) (Table 1). The frontline region included the Sumy, Chernihiv, Kharkiv, Dnipro, and Zaporizhzhia oblasts. The central-western region included the Kyiv, Poltava, Lviv, Rivne, Ternopil, and Ivano-Frankivsk oblasts.
Table 1
Baseline characteristics of participants
Professional burnout was assessed using the Maslach Burnout Inventory (MBI), which includes 22 items to evaluate EE, DP, and PA [20]. Scores were presented as sums of points and percentages of the maximum possible score for each scale.
Burnout level thresholds were defined as follows [18]:
– EE: high (> 27), moderate (17–26), low (< 16), maximum score: 54
– DP: high (> 13), moderate (7–12), low (< 6), maximum score: 30
– PA: high (0–31), moderate (32–38), low (> 39), maximum score: 48
Descriptive statistics, including mean (M), variance, standard deviation (SD), standard error of the mean (SEM), minimum, and maximum values, were used.
Data normality was assessed using the Shapiro–Wilk test. The Levene Test of Homogeneity of Variances determined whether parametric (for homogeneity) or nonparametric (for heterogeneity) statistical tests were used. Comparisons of two groups (sex, facility location) employed t-tests for independent samples. For comparisons of three or more groups, a one-way ANOVA/Scheffé’s test, Median Test, Kruskal–Wallis ANOVA, or chi-square test was applied.
Cluster analysis was used to form and analyse individual profiles of the study participants based on the percentage indicators of the EE, DP, and PA scales.
Results
The data show that during the military conflict, rehabilitation professionals exhibit a moderate level of burnout across all three dimensions: EE (mean 18.11 ± 1.21), DP (mean 7.44 ± 0.61), and PA (mean 37.24 ± 0.75) (Table 2).
Table 2
Average burnout scores among rehabilitation professionals
| PB | n | Mean | Minimum | Maximum | Variance | SD | SEM |
|---|---|---|---|---|---|---|---|
| EE | 112 | 18.11 | 0 | 54 | 164.11 | 12.81 | 1.21 |
| DP | 112 | 7.44 | 0 | 28 | 41.38 | 6.43 | 0.61 |
| PA | 112 | 37.24 | 15 | 48 | 62.76 | 7.92 | 0.75 |
No statistically significant differences were found in the EE, DP, and PA scores among groups categorised by sex, position, work experience, or healthcare facility location (Tables 3–6).
Table 3
Burnout characteristics by position
Table 4
Burnout characteristics by work experience
PB – professional burnout, EE – emotional exhaustion, DP – depersonalisation, PA – professional accomplishment
Table 5
Burnout characteristics by healthcare facility location
Table 6
Burnout characteristics by sex
However, for EE and DP, the highest average values are observed among PRM physicians, and the lowest among PT and OT assistants, which corresponds to a moderate (PRM physicians – EE = 24.25 ± 5.31; DP = 9.13 ± 2.22 and assistants – DP = 6.68 ± 1.22) and low (assistants – EE = 15.60 ± 2.12) level of burnout (Table 3).
The highest levels of burnout (PB) based on the EE, DP, and PA indicators are observed among specialists with more than 15 years of work experience, while the lowest levels are found among those with less than 2 years of experience (Table 4). However, the burnout level is moderate for individuals with extensive work experience and low for younger professionals (less than 2 years of experience).
The average values of EE, DP, and PA among specialists from different regions of Ukraine do not differ significantly. This can likely be explained by the nature of their work: specialists from the central-western region primarily work with severely wounded military personnel who have been transported to safer areas for rehabilitation, while specialists from the frontline region mostly work with patients near their place of residence (military personnel wounded on the frontlines are treated in frontline hospitals, which function as stabilisation points).
No sex differences were identified in our study. However, it is worth noting that the average EE scores are slightly higher among the females compared to the males, while the males have worse DP and PA scores than the females (Table 6).
A cluster analysis revealed individual characteristics of professional burnout, identified individual PB profiles, and grouped the study participants into clusters based on PB scale percentages. The first cluster was characterised by high levels of emotional exhaustion and depersonalisation and low levels of professional accomplishment, corresponding to signs of professional burnout. The second cluster showed moderate levels of emotional exhaustion and depersonalisation and low professional accomplishment, indicating a moderate level of professional burnout. The third cluster exhibited low levels of emotional exhaustion, depersonalisation, and professional accomplishment (Figure 1).
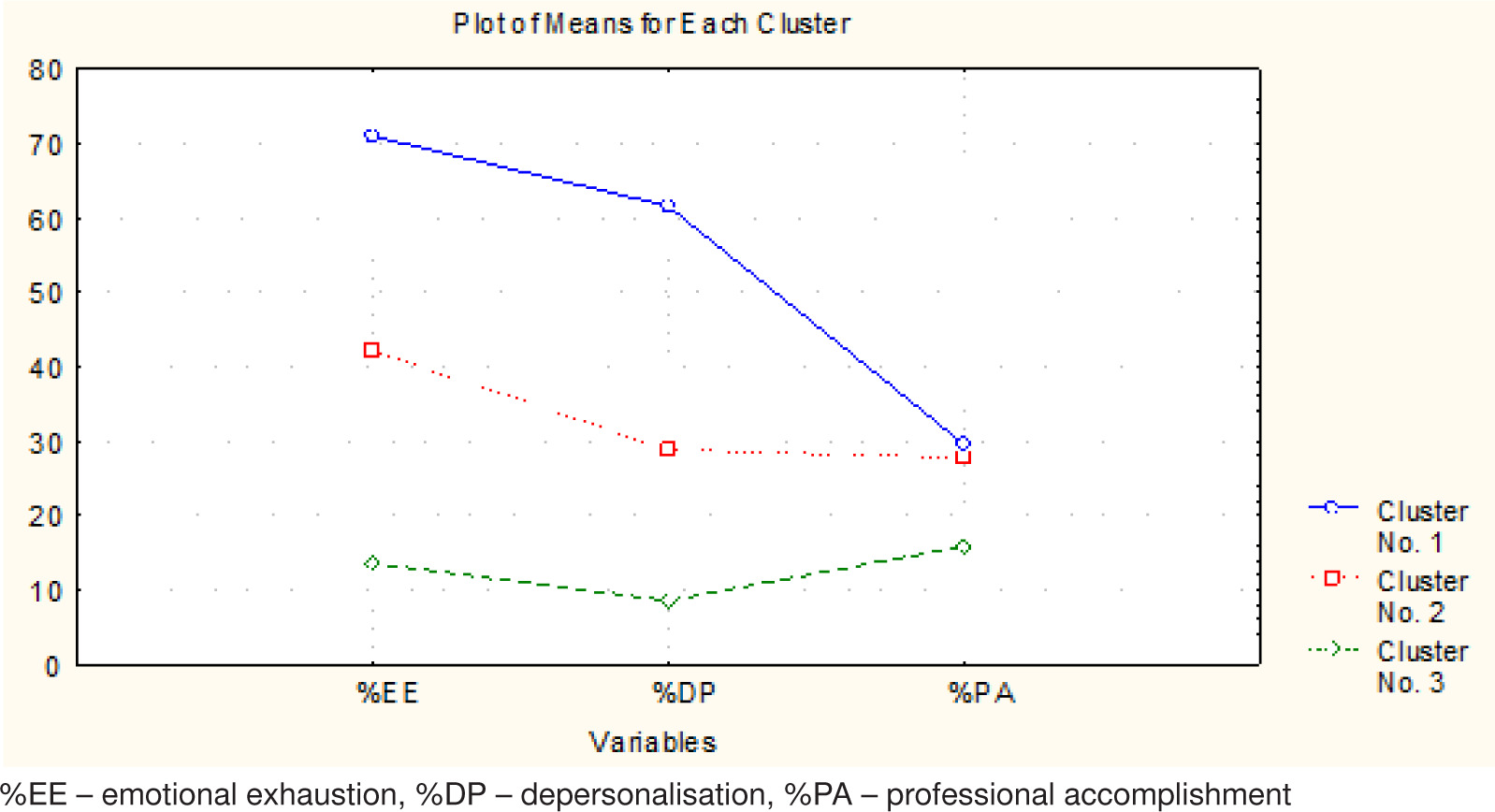
Thus, participants in cluster 1 exhibit high levels of professional burnout, those in cluster 2 demonstrate moderate burn-out, and those in cluster 3 have the lowest levels of burnout.
The characteristics of the emotional exhaustion, depersonalisation, and professional accomplishment indicators as percentages for each cluster are presented in Table 7. The burnout clusters differ significantly from one another in terms of these indicators, as illustrated in Figure 2.
Table 7
Characteristics of emotional exhaustion, depersonalisation, and professional accomplishment indicators by clusters, as percentages
Figure 2
Comparison of burnout clusters by emotional exhaustion, depersonalisation, and professional accomplishment scales
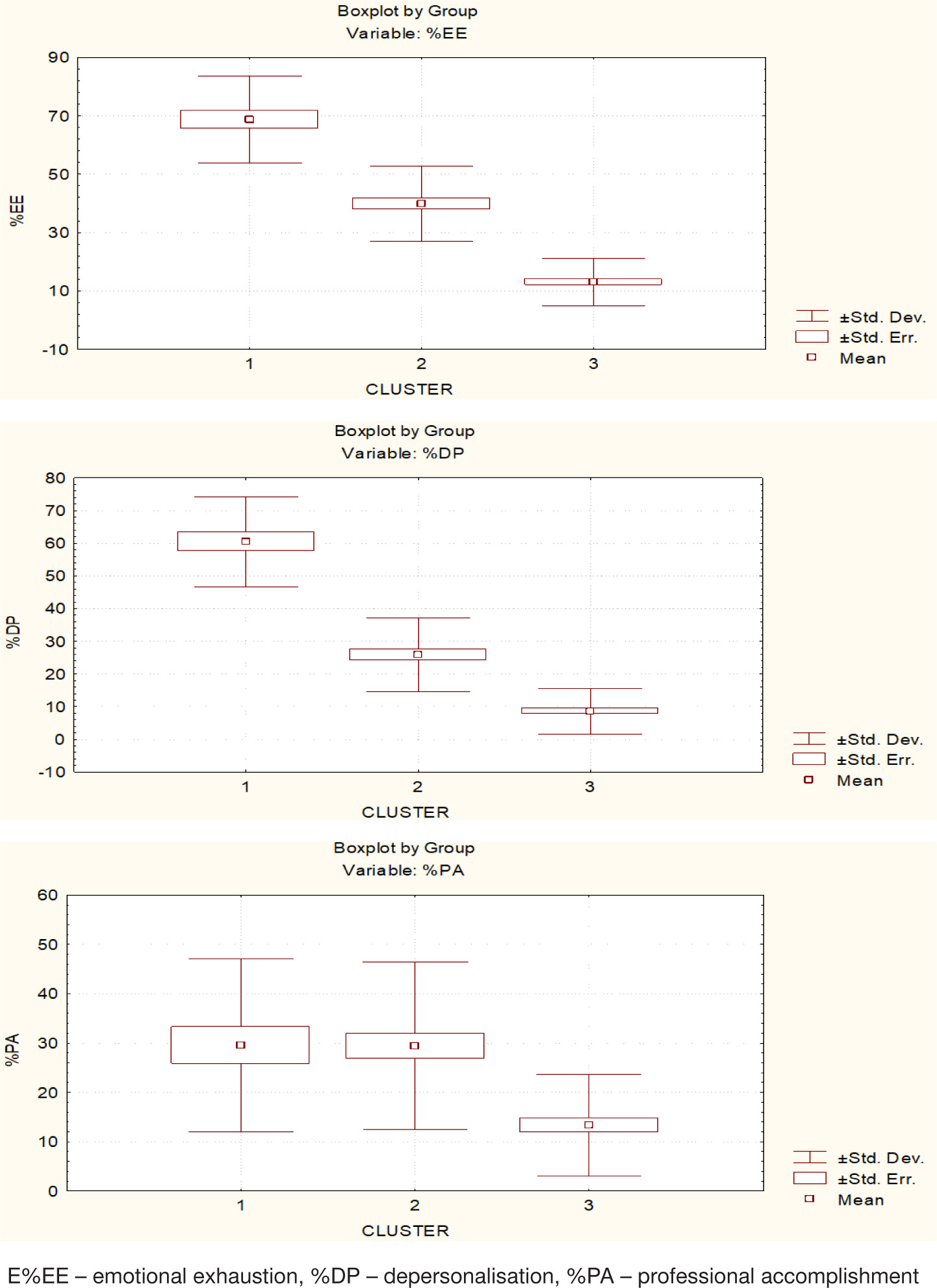
It should be noted that for EE and DP (M ± SEM), representatives of all three clusters differ significantly from one another. For PA, significant differences are observed between the first and third clusters, and the second and third clusters.
The analysis of participants in each cluster by position, work experience, sex, and geographic location revealed no statistically significant differences in distribution. However, there is a noticeable trend of increased professional burn-out risk among rehabilitation professionals with longer work experience (Table 8)
Table 8
Distribution of participants by clusters according to position, work experience, sex, and geographic location in professional burnout clusters, as percentages
The analysis of individual characteristics of PB among rehabilitation professionals in each cluster shows that the majority of professionals belong to the third cluster, which represents those with the lowest risk of professional burn-out (ranging from 37.5% to 50%). Meanwhile, a smaller proportion falls into the first cluster, representing those with the highest risk of professional burnout (ranging from 16% to 25%) (Figure 3).
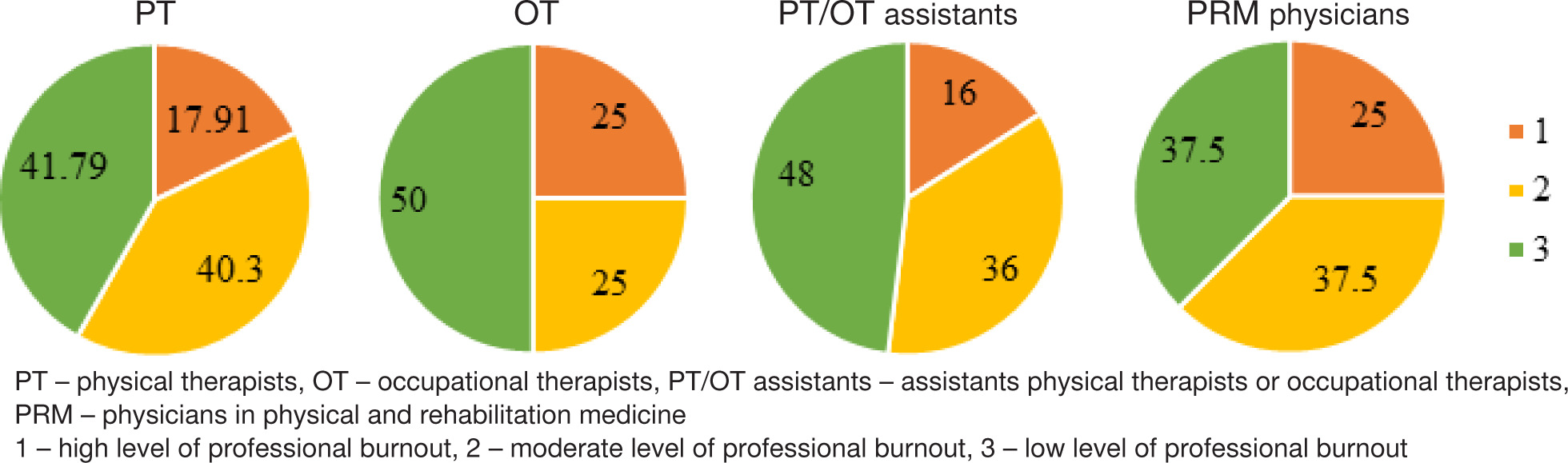
Overall, our results indicate that, based on the individual PB scale indicators, 50% to 65% of rehabilitation professionals exhibit high and moderate levels of professional burnout.
Discussion
Since the study of professional burnout by Maslach et al. [18] and the development of the corresponding assessment tool, numerous results have been obtained for individuals across various professions. Recent studies (2023–2025) on burnout levels among healthcare workers and the factors influencing the development of burnout include works by researchers from the U.S. [21], France [22], Montenegro [23], Spain [24], Poland [18, 25], Italy [17], and other countries.
In the studies of Carmona-Barrientos et al. [26], Janus et al. [25], Kucukakkas et al. [27], and Sargent et al. [10] of PB among healthcare workers, the researchers note a higher degree of PB on the EE scale, and the lowest PB on the PA scale of the MBI, which corresponds to our results.
In a study of burnout among healthcare workers at a military medical centre during wartime by Sargent et al. [10], the MBI scale results were 19.99 for emotional exhaustion, 4.84 for depersonalisation, and 40.56 for personal accomplishment. These findings align with our results on professional burnout among rehabilitation professionals working in frontline and central-western healthcare facilities, except for the depersonalisation scale, where differences were noted. Similar to Sargent et al.’s [10] study, we also found no differences in MBI scale results between professionals from different regions.
In our study, 18.75% of participants exhibited professional burnout. This aligns with findings by Bruschini et al. [28], where 14% of physiotherapists, speech therapists, and occupational therapists showed burnout, and Nozedar and O’Shea’s study [29], where 13% of physiotherapists experienced burn-out. The higher percentage in our study can be attributed to the significant number of severely injured patients requiring rehabilitation due to military actions, which impacts the professionals’ emotional states and increases depersonalisation.
As noted by Venturini et al. [30] in their systematic review and meta-analysis, the combined prevalence of burnout among physiotherapists was 8%, with emotional exhaustion at 27%, depersonalisation at 23%, and low personal accomplishment at 25%. While our findings for EE, DP, and PA are similar (26.79%, 20.54%, and 24.12%, respectively), the overall prevalence of burnout among rehabilitation professionals in our study is twice as high (16.96%).
A high level of burnout among physiotherapists was observed during the COVID-19 pandemic, as shown in various studies [14, 18, 21]. Polish researchers reported the following mean burnout indicators: EE = 32.31, DP = 16.25, and PA = 26.25 [18]. Meanwhile, a study by Carmona-Barrientos et al. [26] found high EE levels among Spanish physiotherapists (mean 21.64 ± 10.57), with low DP (6.57 ± 4.65) and high PA (39.52 ± 5.97) scores.
The results of the research on the relationship between burnout and sex are mixed. Some studies suggest higher burnout rates among males [11, 18, 31]. And, conversely, some show that a higher degree of PB is typical for females [12, 32, 33]. However, our findings do not confirm a higher risk of burnout among females compared to males working as physiotherapists and occupational therapists. In our study, the DP and PA mean values for males were slightly worse than those for females, similar to findings by the Polish researchers in Pniak et al. [18].
Professional experience can also influence burnout levels. Pniak et al. [18] found the highest EE scores among physiotherapists with over 20 years of experience, while those with 10–15 years of experience had the highest DP and PA scores. Another study in Cadiz (Spain) identified a link between high stress levels and more than 10 years of work experience [26]. Similarly, Elhadi et al. [34] found a connection between anxiety symptoms and the work experience of healthcare professionals.
The findings of Klingemann and Wieczorek [4] emphasise that professional burnout can have serious consequences not only for the affected professionals but also for their colleagues and patients, ultimately leading to a reduction in the overall effectiveness of patient rehabilitation.
Thus, studying burnout among rehabilitation professionals and the modifiable factors influencing its development is necessary to identify effective prevention strategies. Analysing individual burnout profiles appears to be a more promising approach for this purpose.
Limitations
This was a cross-sectional study, making it impossible to establish causal relationships between the indicators. Our sample was randomly formed from various regions of Ukraine, so interpreting the results requires caution when generalising conclusions to all rehabilitation professionals in the country. Additionally, the sample size was relatively small, and a larger sample might have led to different proportions in groups based on position and work experience. The results reflect only the current state of professional burnout among rehabilitation professionals and do not account for changes over time.
Conclusions
The average data obtained in our study indicate that, during military conflict, rehabilitation professionals generally exhibit a moderate level of burnout across all three scales: EE (emotional exhaustion), DP (depersonalisation), and PA (personal accomplishment). Unmodifiable factors such as sex, work experience, and the location of the facility do not significantly influence the indicators of emotional exhaustion, depersonalisation, or professional accomplishment. However, the analysis of individual burnout profiles allowed us to identify groups with high and moderate levels of emotional exhaustion and depersonalisation, low levels of professional accomplishment, and a group with low levels of all three indicators.
It was shown that 50% to 65% of Ukrainian rehabilitation professionals working under conditions of military conflict have high or moderate levels of professional burnout.
This study can be considered a pilot, and further research with a larger sample size is needed. Nevertheless, the findings highlight the necessity of developing burnout prevention strategies for rehabilitation professionals based on the evaluation of individual burnout profiles.