Introduction
Rotator cuff disorders are extremely common, affecting around 6.8% to 22.4% of the population over the age of 40 [1]. Shoulder pain represents a significant musculoskeletal condition, with up to 50% of the population encountering at least one occurrence annually [2]. The most prevalent cause of shoulder pain and weakness is rotator cuff tendinopathy (RCT) [3]. It occurs when tendons become irritated, usually from high pressure placed on the acromion or, less often, issues within the tendon itself; Via et al. [4]. The pathoetiology is multifactorial, involving external and internal mechanisms, along with environmental factors [3]. External factors include direct trauma (falls, accidents) and overuse from repetitive movements (lifting, pushing, pulling, throwing). Internal factors include reduced blood supply, age-related degeneration, and tendon calcification [4]. The probability of RCT increases with factors like age over 50, diabetes, and smoking [5].
The management of RCT is mainly conservative. Electro-therapies, such as therapeutic ultrasound [5], low-level laser therapy, transcutaneous electrical nerve stimulation, and pulsed electromagnetic field therapy, are effective at relieving symptoms [6]. Exercise therapy is efficient in decreasing the pain level and improving function [7].
Pilates exercises have a positive influence on muscle strength, tolerance, posture, stretchability, body physique, balance and proprioception in patients with shoulder problems [8]. Pilates exercises facilitate compressive and decompressive forces on the connective tissues that help in conditions such as osteoporosis, cartilage and ligamentous tears, disc prolapse and myofascial pain syndrome [9]. Diaphragm manual therapy is another effective way to improve shoulder mobility, helping reduce pain and enhance movement in rotator cuff patients [10].
The shoulder and diaphragm are connected through the myofascial system, with trunk fascia extending to the upper limbs. The diaphragm links to the pectoral muscle, latissimus dorsi, and subscapularis, as well as to the shoulder via mediastinal tissues like the pericardium and pleura. Additionally, a neural connection exists between the phrenic and suprascapular nerves, known as the ‘phrenic-suprascapular communication’ [10].
Given the benefits of Pilates for shoulder function and pain, and diaphragm manual therapy for pain and mobility, it is valuable to explore their combined effect. This study aimed to assess their impact on pain intensity, pain threshold, shoulder strength, and overall function in rotator cuff tendinopathy patients.
Subjects and methods
Subjects
This study was a prospective, randomised controlled trial with a pretest–posttest design. Sixty patients of both sexes participated in this study and were referred for physical therapy by orthopaedist with the diagnosis of chronic rotator cuff tendinopathy that has lasted more than 3 months [9]. This study was conducted in the primary care health unit in the sixth district of the Sixth of October city, affiliated with the Egyptian Ministry of Health, from May 2023 to March 2024. Subjects fulfilled the following criteria (a) age range from 40 to 60 years, either male or female [11]; (b) BMI within the normal range between 18.5 and 24.9 [12]; (c) they complain of shoulder pain located at the upper outer arm; the pain was aggravated by resistance during abduction and/or lateral rotation, reaching, pushing, pulling, lifting, elevating the arm above the shoulder level, or lying on the affected arm [9]. Subjects were excluded according to the following criteria: (a) stiff shoulder such as adhesive capsulitis, previous dislocation or sublation; (b) previous shoulder surgery or recent thoracic surgery; (c) glenohumeral joint or acromioclavicular joint degeneration; (d) any deformity of the spine; (e) heavy smokers; (f) history of thyroid disorders or cardiopulmonary pathology; (g) cognitive impairment [9].
Sample size
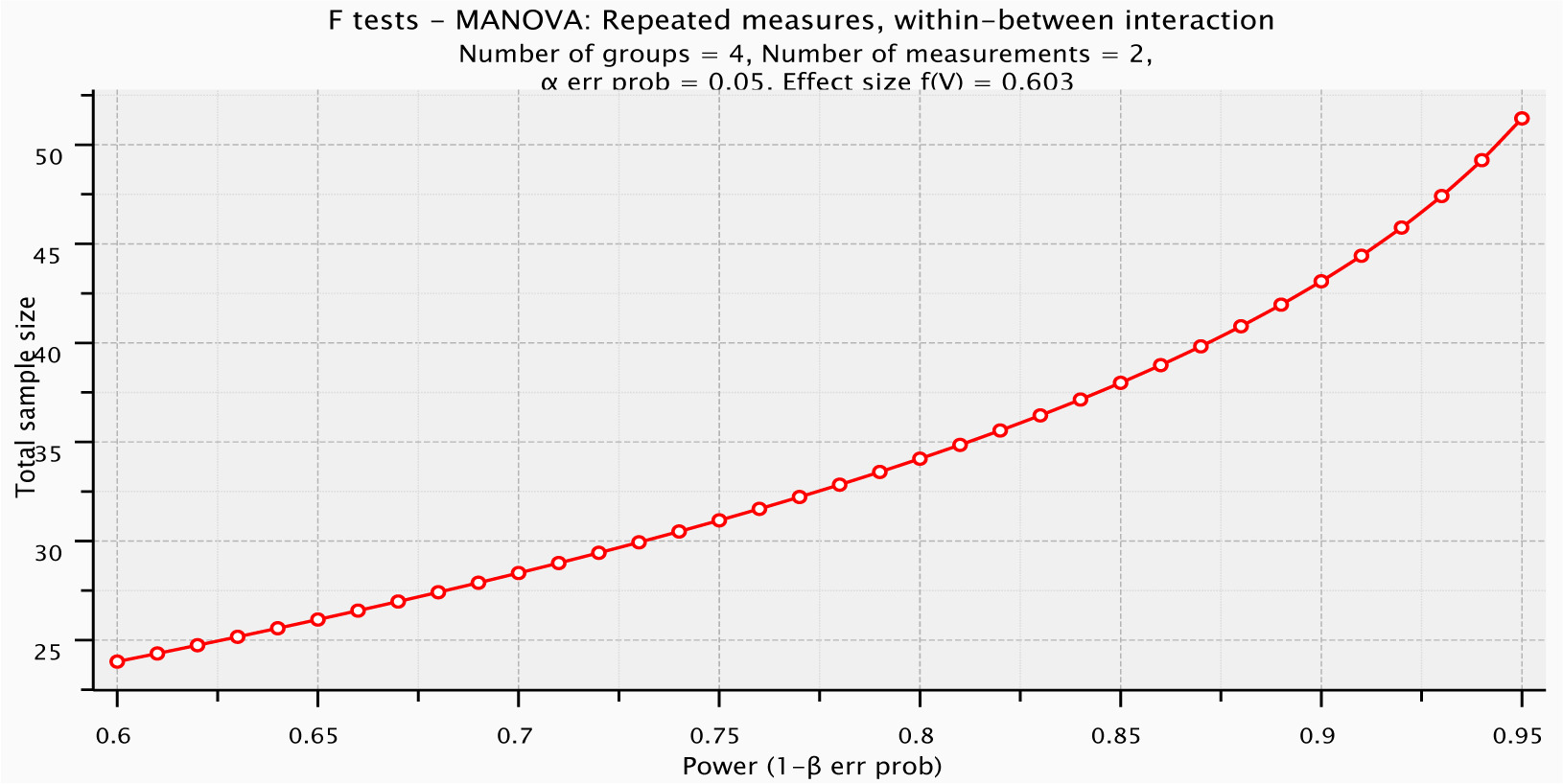
The appropriate sample size was calculated before starting this study to reduce the possibility of a type II error. The G*Power software (version 3.0.10) was used to calculate the minimal estimated sample size. The minimum proper sample size was 52 subjects with 95% power at = 0.05, number of measurements = 2 (pretest–posttest), for 4 groups, and effect size = 0.603 using F-test MANOVA within and between interaction effects. Eight more subjects were then added (15% drop out), so the total sample size was 60 (Figure 1).
Randomisation
Subjects were randomly assigned equally to 4 groups of 15 subjects each. The coin-flip method over two rounds was used on blinded subjects to avoid selection bias and limit the variability among the groups. The randomisation was done by a blinded researcher who was not involved in the data collection. When the therapist opened the envelope containing the coin-flip assignment, therapy was started based on group allocation (Figure 2).
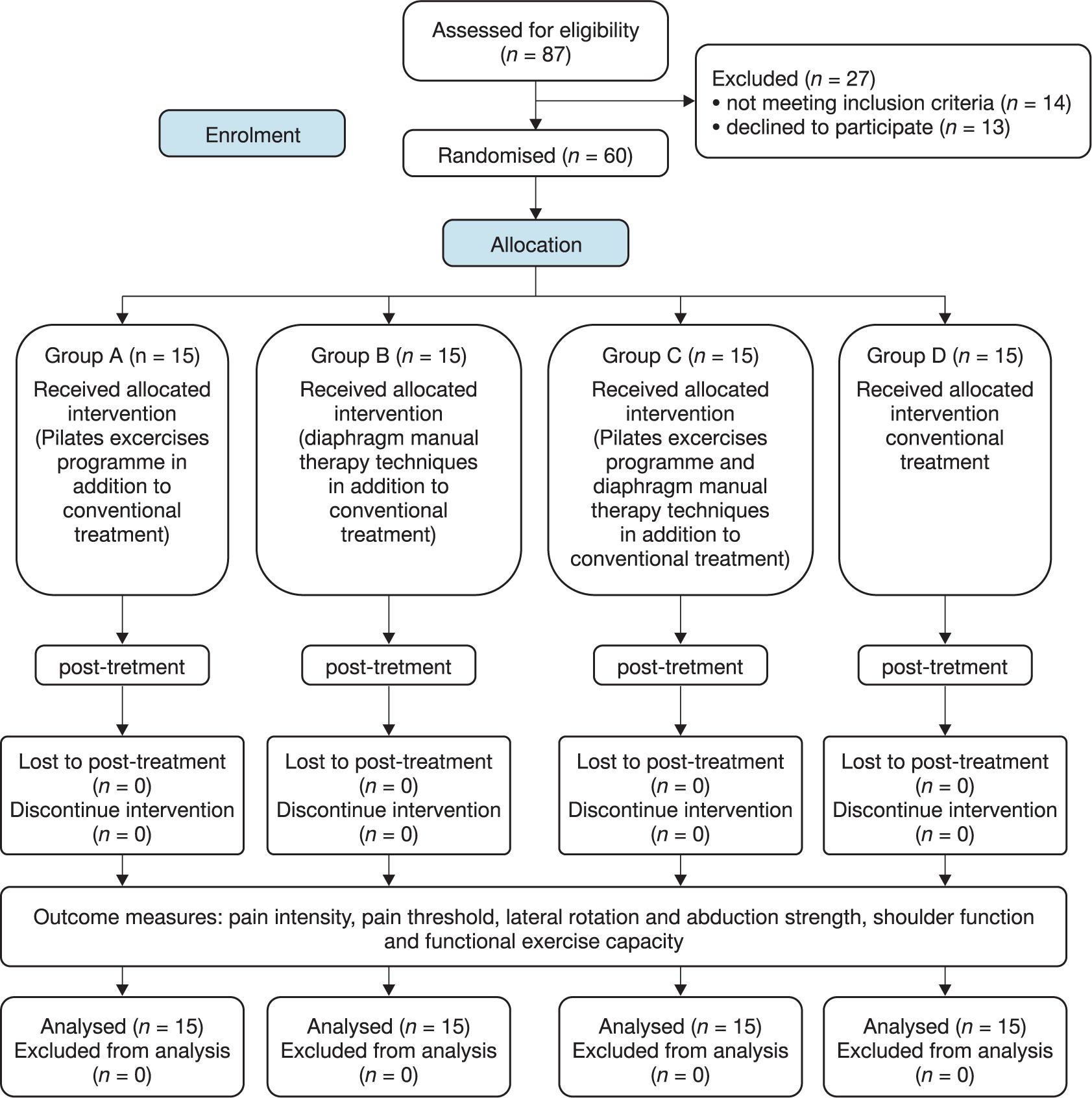
Subjects received 24 treatment sessions in the form of three sessions per week for 8 weeks. Group A: (study group) received a Pilates exercise programme in addition to conventional physical therapy treatment for RCT, Group B: (study group) received diaphragm manual therapy techniques and conventional physical therapy treatment for RCT, Group C: (study group) received diaphragm manual therapy techniques and a Pilates exercise programme in addition to conventional physical therapy treatment for RCT, and Group D: (control group) received conventional physical therapy treatment for RCT.
Statistical analysis
Data were screened for the normality assumption, homogeneity of variance, and presence of outliers. The Kolmogorov–Smirnov test for normality showed that all measured variables were normally distributed except for pain intensity, so a mixed-model MANOVA test was used to analyse the parametric variables. The Kruskal-Wallis and Wilcoxon-Wallis tests were used to analyse the pain intensity. Statistical analysis was conducted using SPSS for Windows, version 20 (SPSS, Inc., Chicago, IL). The alpha level was set at 0.05.
Procedures
Assessment procedures
Pain intensity assessment: it was measured via the visual analogue scale (VAS) which is valid and reproducible tool [13]. The scale is 10-cm-long measuring tool that ranges from 0 = ‘no pain’ to 10 = ‘excruciating pain’ [14]. Each patient was asked to choose their level of pain intensity from this 0 to 10. The pain was assessed at rest and during activities. The measurements were taken before and after the end of the intervention programme [15].
Pain Threshold Assessment: Pressure algometry (Baseline Mechanical Push/Pull Dynamometer, made in the USA) was used to measure sensitivity to pain [16]. It is a valid and reproducible instrument [17]. It was used at the supraspinatus tendon [18], xiphoid process (supine), and C4 spinous process (prone) [19, 20]. Measurements were taken three times at 15 s intervals, and the mean (kg/cm2) was calculated. Subjects indicated when pressure turned to pain, with the algometer held perpendicular to the site [21].
Shoulder muscle strength assessment: The muscle strength was measured via a handheld dynamometer (LAFAYETTE Digital Hand-Held Manual Muscle Tester MMT, Model number 01163, made in the USA). It showed excellent reliability and moderate-to-good validity [22].
(a) Shoulder 90° abduction with 90° external rotation: In a standing position resting on a wall with the shoulder at 90° abduction and 90° external rotation, the elbow flexed 90°. The dynamometer was stabilised against the wall. The patient was asked to press against the wall. Each contraction lasted 3 s, with three trials, one minute of rest was given between trials, and verbal encouragement ensured maximum effort [23].
(b) Shoulder 45° abduction: supine position, the affected shoulder was abducted to 45° with the elbow extended and palm facing the leg. A handheld dynamometer was placed just above the ulnar styloid. Each contraction lasted 3 s, with three trials, one minute of rest between trials, and verbal encouragement to ensure maximum effort [24].
Shoulder function assessment: The shoulder function level was measured via the Arabic version of the Disabilities of the Arm, Shoulder and Hand (DASH-Arabic) questionnaire [25]. It is a valid, reliable and sensitive upper extremity outcome measure for subjects whose native language is Arabic; it can be used to record subject condition and outcomes and contribute to evidence-based practice [26].
Exercise capacity assessment: The exercise capacity level was measured via the 6-minute walk test. It is a valid and reliable measure of physical tolerance and overall physical functional capacity in adults [27].
All measurements were recorded before and after the eight-week intervention, covering pain intensity, pain threshold, shoulder function, muscle strength, and functional capacity.
Interventions procedures
(1) Pilates exercises: A 3–4 min warm-up and cool-down before the exercise
Ribcage arms. Starting position: supine with the knees flexed and arms extended beside the body. Action: raise the arms towards the ears while inhaling, then return to the starting position while exhaling. Perform 5–10 repetitions [9].
Snow angel. Starting position: supine with flexed knees, arms extended beside the body, and the palms facing the ground. Action: abduct the arms in the direction of the head. You need to turn the palms up while moving. Perform 5–10 repetitions [9].
Pinwheel exercise. Starting position: lie on the unaffected side with flexed knees and both arms straight in front of your body and your palms facing each other. Action: move the affected arm to make a whole circle and return to the starting position. Turn the palms up while moving. Perform 5–10 repetitions [9].
Telescope arms. Starting position: lie on the unaffected side with flexed knees and both arms straight in front of your body and your palms facing each other. Action: slide the affected arm over the unaffected one by flexing your elbow and hyperextend the shoulder and return to the starting position. Perform 5–10 repetitions [9].
Swimming. Starting position: prone position with forward flexion of the arms and straight legs. Action: flex the right arm while extending the left leg and vice versa. Perform 5–10 repetitions [9].
Single arm single leg extensions. Starting position: Crawling position. Action: flex the right arm while extending the left leg and vice versa. Perform 5–10 repetitions [9].
Quadruped shoulder flexion. Starting position: crawling position. Action: flex the affected arm and return to the starting position. Perform 5–10 repetitions [9].
(2) Diaphragm manual therapy techniques
1. Seated diaphragm stretch: the subject sits upright, takes deep breaths, and exhales. During exhalation, the therapist grips the lower ribs and costal margins, deepening the stretch with each breath for 5–7 min [28].
2. Supine diaphragm release: the subject lies on their back with relaxed limbs. During exhalation, the therapist applies downward pressure with their thumbs, following the diaphragm’s movement for 5 respiratory cycles [29].
3. Lateral diaphragm stretch: the subject lies on the unaffected side with the affected shoulder relaxed. The therapist presses the internal costal cartilage and ribs obliquely towards the affected shoulder during inhalation, maintaining pressure on exhalation to prevent descent. This is repeated for 15 respiratory cycles [30].
(3) Conventional physical therapy treatment for RCT Therapeutic ultrasound parameters: 5 min, 1 MHz, 1.5 W/cm2. Brand: Astra, model Etius U, made in Poland. Hot Pack therapy was applied for 20 min to cover the affected shoulder [9].
The subjects were asked to do the exercises under therapist supervision. The exercises utilised in the study were the pendulum exercise, corner stretch, upper trapezius self-stretching, active range of motion exercises in the flexion, abduction, internal, external rotation direction, and a home exercise programme [8, 31].
Pendulum exercises (Codman exercises). Starting position: bending the trunk forward with the affected arm hanging downwards while standing. Action: move the arm forward and backward, from side to side and in a circular movement using the momentum of the trunk without contracting the shoulder muscles. Perform 10 repetitions [32].
Flexion. Starting position: sitting in an erect position with the arm beside the body. Action: the patient moves the arm anterior and returns it to the starting position. Perform 10 repetitions [31].
Extension. Starting position: sitting upright with the arm beside the body. Action: the patient move the arm posterior and returns it to the starting position. Perform 10 repetitions [31].
Abduction. Starting position: sitting in an erect position with the arm beside the body. Action: the patient moves the arm away from the midline and returns it to the starting position. Perform 10 repetitions [31].
Internal and external rotation. Starting position: sitting in an erect position with the elbow flexed 90° and the palm of the hand resting over the abdomen. Action: the patient moves the forearm away from the midline and returns it to the starting position. Perform 10 repetitions [31].
Internal and external rotation from 90° abduction. Starting position: standing in an erect position with the back resting on a wall, elbow flexed 90°, shoulder abducted 90° and the dorsum of the hand resting on the wall. Action: the patient moves the forearm anterior to try to touch the wall with the palm and returns it to the starting position. Perform 10 repetitions [31].
Corner stretch. Starting position: standing facing a wall corner or open doorway, shoulder abduction and external rotation 90°, elbows flexed 90° and hand resting on a wall. Action: push the body slowly forward towards the corner until a stretch is felt in the anterior part of the shoulder. Hold for 10 s, relax for 10 s, repeat 3 times [33].
Upper trapezius self-stretching. Starting position: sitting in an erect position with one hand above the head. Action: the patient slowly pulls the head in the direction of the shoulder, holds the position and releases it slowly. Hold for 10 s, relax for 10 s, repeat 3 times [31].
Home exercise programme. It included the same exercises as the supervised programme. Subjects were instructed to perform them 1–2 times/day within a pain-free ROM and to stop immediately if the pain worsened.
Results
Subject characteristics
There was no significance difference between groups in the mean values of age (years), weight (kg), height (m) or body mass index (BMI, kg/cm2) (p = 0.078, 0.091, 0.082 and 0.141, respectively), and there was no significant difference between groups in sex distribution or affected shoulder distribution (p = 0.193 and 0.720, respectively), as shown in (Table 1).
Table 1
Mean values of demographic characteristics of the group
Treatment results of pain VAS (cm)
The post-treatment analysis of pain intensity using the VAS (cm) revealed no significant differences between the four groups in pain at rest, both before and after treatment (p = 0.948 and 0.084, respectively). However, all groups showed a significant within-group improvement (p = 0.001) with a 100% reduction in pain intensity at rest. Regarding pain during activity, there was no statistically significant difference in pre-treatment values between the groups (p = 0.869), while post-treatment results showed a significant difference (p = 0.032). All groups demonstrated significant reductions in pain during activity (p = 0.001), with percentage improvements of 60% in group A, 40% in group B, 100% in group C, and 50% in group D. Post-hoc analysis revealed significant differences between group B and group C (p = 0.023), and between group C and group D (p = 0.005), favouring group C in both cases (Table 2).
Table 2
Comparison between pre- and post-treatment mean values of pain intensity (VAS cm) at rest and during activity
Post-treatment pressure algometry (kg) results of pain threshold
Post-treatment results of pain threshold (kg) at supraspinatus
There were no statistically significant differences between groups A and B (p = 1), between groups A and C (p = 0.120), between groups A and D (p = 1) or between groups B and D (p = 0.828). In contrast, there was statistically significant differences between groups B and C (p = 0.007) in favour of group C, and between groups C and D (p = 0.034) in favour of group C (Table 3).
Table 3
Comparison between pre- and post-study mean values of pain threshold (kg) of supraspinatus between and within groups
Post-treatment results of pain threshold (kg) at xiphoid
There were no statistically significant differences between groups A and B (p = 1), between groups A and D (p = 0.602), or between groups B and D (p = 0.806). In contrast, there were statistically significant differences between groups A and C (p = 0.001) in favour of group C, between groups B and C (p = 0.001) in favour of group C, and between groups C and D (p = 0.044) in favour of group C (Table 4).
Table 4
Comparison between pre- and post-study mean values of pain threshold (kg) of xiphoid between and within groups
Post-treatment results of pain threshold (kg) at C4
There were no statistically significant differences between groups A and B (p = 1), between groups A and D (p = 1), or between groups B and D (p = 1). In contrast, there were statistically significant differences between groups A and C (p = 0.040) in favour of group C, between groups B and C (p = 0.001) in favour of group C, and between groups C and D (p = 0.001) in favour of group C (Table 5).
Table 5
Comparison between pre- and post-study mean values of pain threshold (kg) at C4 between and within groups
Post-treatment results of muscle strength (kg)
Post-treatment muscle strength (kg) results of external rotation strength at 90° abduction and 90° external rotation
There were no statistically significant differences between groups A and C (p = 1) or between groups B and D (p = 0.398).
In contrast, there were statistically significant differences between groups A and B (p = 0.001) in favour of group A, between groups A and D (p = 0.033) in favour of group A, between groups B and C (p = 0.001) in favour of group C, and between groups C and D (p = 0.016) in favour of group C (Table 6).
Table 6
Comparison between pre- and post-study mean values of muscle strength (kg) of external rotators from shoulder abduction between and within groups
Post-treatment muscle strength (kg) results of shoulder abductors at 45°
There were no statistically significant differences between groups A and C (p = 1) or between groups B and D (p = 0.398). In contrast, there were statistically significant differences between groups A and B (p = 0.001) in favour of group A, between groups A and D (p = 0.001) in favour of group A, between groups B and C (p = 0.001) in favour of group C, and between groups C and D (p = 0.001) in favour of group C (Table 7).
Table 7
Comparison between pre- and post-study mean values of muscle strength (kg) of abductors between and within groups
Post-treatment DASH scores of upper extremity functional disability
There were no statistically significant differences between groups A and C (p = 1), between groups A and D (p = 1), between groups B and D (p = 0.066) or between groups C and D (p = 1). In contrast, there were statistically significant differences between groups A and B (p = 0.001) in favour of group A, and between groups B and C (p = 0.009) in favour of group C (Table 8).
Table 8
Comparison between pre- and post-study mean values of DASH scores between and within groups
[i] Data are represented as mean ± standard deviation DASH – disabilities of the arm, shoulder and hand p-value1 – significance level between groups, p-value2 – significance level within group, p-value3 – significance level for post hoc test % of change – percent of statistical difference between pre- and post-treatment results; * significant
Post-treatment 6MWD (m) results of functional exercise capacity
Comparison between groups
There were no statistically significant differences between groups A and B (p = 1), between groups A and C (p = 1), between groups A and D (p = 0.133), between groups B and C (p = 0.539) or between groups B and D (p = 1). In contrast, there was a statistically significant difference between groups C and D (p = 0.030) in favour of group C (Table 9).
Table 9
Comparison between pre- and post-study mean values of 6MWD (m) between and within groups
[i] Data are represented as mean ± standard deviation. 6MWD – 6 minutes walk distance p-value1 – significance level between groups, p-value2 – significance level within group, p-value3 – significance level for post hoc test % of change – percent of statistical difference between pre- and post-treatment results; * significant
Discussion
This study aimed to examine the effects of Pilates and diaphragm manual therapy on chronic rotator cuff tendinopathy, evaluating pain, muscle strength, shoulder function, and exercise capacity. No significant differences were found in resting pain (p = 0.084), but group C showed greater pain relief during activity compared to groups B (p = 0.023) and D (p = 0.005). Group C also had higher pain thresholds at the supraspinatus (p = 0.007), xiphoid (p = 0.001), and C4 (p = 0.001). Shoulder external rotation strength (p = 0.001), function (p = 0.009 compared to group B), and exercise capacity (p = 0.030 compared to group D) improved most in group C, suggesting its treatment was the most effective.
The findings of this study highlight the clinical value of using Pilates exercises and diaphragm manual therapy techniques in managing rotator cuff tendinopathy (RCT). These approaches, whether applied individually or in combination, demonstrated notable improvements in patient outcomes, potentially reducing the reliance on nonsteroidal anti-inflammatory drugs and analgesics. The simplicity and accessibility of the exercises, requiring no specialised equipment, also makes them highly practical for use in outpatient physical therapy settings. This supports their integration into routine rehabilitation protocols for RCT patients.
Pain
Similar results were obtained by Akbaş et al. [9], who compared Pilates exercise and conventional treatment for RCT. The Pilates group received an exercise programme focused on the shoulder complex, while the other group received conventional therapy (hot-pack, ultrasound and home exercise programme 5×/week). The study evaluated the pain intensity level at night and during movements, shoulder function level, general health level, and anxiety level. All variables advanced in both groups. Pain (flexion and abduction) remained in the control group but improved in the Pilates group.
Similar results were also obtained by Şahin et al. [34], who found diaphragmatic breathing and mobilisation effective in reducing shoulder pain and improving quality of life. They studied 72 individuals with shoulder pain divided into three groups: control, mobilisation, and breathing. Using VAS for pain and quality of life assessed with Short Form-36 (SF-36) for quality of life, they found diaphragmatic mobilisation and breathing exercises effective in reducing pain and enhancing quality of life.
Karkousha et al. [35] investigated 40 female participants with upper cross syndrome, divided into a control group A receiving traditional physical therapy – stretching, strengthening, and postural correction – and an experimental group B receiving Pilates exercises. Both groups had sessions twice a week for four weeks. The results showed that Pilates was more effective in improving spinal curvature, balance and function, and in reducing pain. Similarly, the current study found that Pilates effectively reduced pain.
Elhafez et al. [36] conducted a study on 60 participants (aged 18–25) with forward head posture, randomly assigned to three groups: group A received Pilates mat and postural correction exercises, group B received cervical stabilisation and postural correction, and group C received only postural correction. Interventions were done three times a week for 12 weeks. Assessments included craniovertebral angle, pain intensity (VAS), neck function by the Arabic neck disability index (ANDI), and muscle activity by surface electromyography (sEMG). The results showed that both Pilates mat and cervical stabilisation exercises were effective, with Pilates being more beneficial. These findings are consistent with the current study, which also reported significant pain reduction following Pilates exercises.
Shoulder strength and function
Kolomiitseva et al. [37] studied the effects of 12 weeks of Pilates (three sessions per week) on 18 sedentary middle-aged women. Pilates improved shoulder girdle strength and mobility, particularly flexion, aligning with the current study’s findings. A pilot study by Keays et al. [38] on four women recovering from breast cancer treatments found that Pilates may safely improve shoulder abduction, external rotation, and overall physical and mental health.
Diaphragm manual therapy techniques were found effective by Fernández et al. [10] in reducing pain and improving shoulder movement compared to active diaphragm mobilisation and ischemic compression. Pain, ROM, and pressure algometer assessments supported the efficacy of indirect shoulder treatment through diaphragm therapy.
The results of the study accord with Atılgan et al. [8], who found significant improvements in shoulder pain (VAS) and function assessed by the Shoulder Pain and Disability Index (SPADI). It confirms that clinical Pilates is more effective than conventional exercises for improving shoulder function in patients with shoulder pain. Our results align with Akbaba et al. [31], who studied 53 rotator cuff tear patients. They compared two groups: (1) conventional treatment with ischemic pressure on active trigger points, and (2) conventional treatment. Assessments included ROM (goniometer), function [DASH and ASES (American Shoulder and Elbow Surgeons Standardized Shoulder Assessment)], and anxiety/depression by the Hospital Anxiety and Depression Scale (HADS). Both groups showed significant improvement, with no clear advantage for group 1. Rotator cuff weakness may cause instability, leading to trapezius fatigue. Conventional therapy restores flexibility, strength, and shoulder balance.
Similar findings were reported by Mohamed et al. [39], who investigated the effects of adding Pilates exercises to a traditional physiotherapy programme. In their study, group A received both Pilates and traditional physiotherapy, while group B received only the traditional physiotherapy programme. The study included 76 patients aged 20 to 40 years with second-degree (partial-thickness) thermal burns affecting the lower limbs. Muscle strength and balance were assessed using a handheld dynamometer (HHD) and the Berg Balance Scale (BBS). The results indicated that incorporating Pilates exercises significantly improved lower limb muscle strength, balance, and overall functional status during the rehabilitation process for these patients.
Exercise capacity
The results of our study showed significant improvement in exercise capacity in the Pilates group, which stands in agreement with a study done by Guclu et al. [40]. They studied the effect of Pilates exercise done 3 times per week for 8 weeks on multiple sclerosis (MS) patients and compared it with a control group. The 6-minute walk test was utilised to evaluate functional exercise capacity level. The results showed significant improvement in MS group. A study by Rocha et al. [41] investigated the effect of a manual diaphragm release technique on the management of patients with chronic obstructive pulmonary disease. They used the 6-minute walk test to evaluate the exercise capacity, and the results showed significant improvement in diaphragmatic mobility, exercise capacity and inspiratory capacity. This study agreed with our results, which showed improvement of the exercise capacity due to manual diaphragm release.
Clinical impact
This study provides strong support for the application of Pilates and diaphragmatic mobilisation as safe and effective non-invasive strategies in the treatment of shoulder dysfunction and pain. The observed benefits, including increased shoulder mobility, reduced discomfort, and enhanced quality of life, emphasise the value of incorporating clinical Pilates and diaphragm-centred techniques into rehabilitation plans for patients with shoulder-related issues.
Notably, Pilates was particularly effective in improving shoulder girdle strength and mobility, especially in the flexion movement, corroborating earlier research. These results point to Pilates as a beneficial tool for re-establishing muscle balance, refining posture, and promoting joint stability. Its gentle and adaptable nature makes it well-suited for use among sedentary or middle-aged individuals, and its structured approach enables safe and progressive use in therapeutic settings.
The success of diaphragm-based interventions in alleviating shoulder pain underlines the importance of addressing respiratory and postural elements in musculoskeletal therapy. Employing these techniques may lead to better clinical outcomes, minimise the need for medication, and support long-term functional improvement.
Limitations
This study’s potential limitations include the short 8-week length of the intervention, making long-term effects uncertain, and the small sample size, limiting the generalisability of the results.
Conclusions
Based on the scope and findings of this study, it can be concluded that a Pilates exercise programme combined with diaphragm manual therapy is more effective than just one of them in relieving pain, promoting and improving the functional activity of shoulder, and increasing muscular strength in cases of rotator cuff tendinopathy.