Introduction
Low back pain (LBP) is one of the most prevalent musculoskeletal disorders, affecting millions of individuals worldwide. The majority of people experience a significant episode of LBP by the time they turn thirty years old. LBP is the most common cause of musculoskeletal problems. It is a leading cause of disability and often results in significant economic and social burden [1]. The complexity of LBP is partly due to the involvement of multiple structures, including muscles, ligaments, and the spine itself, all of which play a role in providing stability and movement. The lower back is known to be supported and stabilised by muscles such as the quadratus lumborum (QL), psoas, multifidus, and erector spinae. Among the many muscles contributing to spinal stabilisation, the QL is a key but often overlooked muscle in the context of LBP [2]. The QL, a deep muscle located in the lower back, plays an essential role in stabilising the lumbar spine, particularly during movements that require lateral flexion or rotation. It functions to resist shear forces that could otherwise destabilise the spine, which is especially important during activities like lifting, bending, or twisting. Despite its crucial role, the QL is often overlooked in the management of LBP, partly because it is not as easily accessible or noticeable as other larger muscle groups. Many individuals focus on strengthening more prominent muscles such as the rectus abdominis or the erector spinae, neglecting the deeper stabilisers like the QL. However, dysfunction or weakness in the QL can contribute to imbalances and increased strain on the spine, potentially leading to or exacerbating LBP. In fact, poor activation or tightness in the QL can also affect the pelvis and the diaphragm, further complicating spinal mechanics [3]. The QL muscle is inserted on the inter-transversal muscles, whereas the iliopsoas muscle is positioned anterior to the inter-transverse muscles on the transverse apophysis of the vertebrae, indicating an anatomical link between the two [4]. The deep sheath of the thoracolumbar fascia divides the iliopsoas and the QL [5]. When diagnosing and treating LBP, the psoas muscle is crucial to take into account because of its function as a primary hip flexor and spine stabiliser [6, 7].
Literature concerning the correlation of the psoas muscle as a source of LBP has shown hypertrophy and tightness of the psoas muscle [8–10]. A tight iliopsoas frequently presents a diagnostic challenge and might manifest as a variety of clinical situations involving LBP [11]. The two layers (anterior and posterior) of the QL play a crucial role in controlling pelvic movement in the coronal plane [12]. Tightness of the QL affects the iliopsoas as both the muscles are anatomically linked [13]. A tight QL and iliopsoas cause excessive anterior pelvic tilt. Studies reported a significant increase in the length of the iliopsoas muscle, and post trigger point release of the QL in asymptomatic individuals [14, 15].
It has been suggested that muscle ultrasonography is an effective method for measuring muscle length. A growing acceptability of the technology in musculoskeletal evaluations may be indicated by the increase in the number of muscle ultrasonographic (USG) studies appearing in the literature [16]. Ultrasonographic evaluation of the iliacus muscle is a valuable tool in assessing hip function and diagnosing related pathologies. This imaging modality offers a non-invasive method to measure muscle size and detect abnormalities, which is crucial for effective treatment planning [17].
Physical therapists use a variety of methods for the management of non-specific low back pain (NSLBP), such as manual therapy, exercises, spinal manipulation, and therapeutic modalities [1]. Instrument-assisted soft tissue mobilisation (IASTM) is a tool gaining popularity in the treatment of soft tissue and myofascia while enhancing range of motion and function [18, 19]. IASTM uses specialised tools, like in the Graston Technique, cupping, vibrators, and Gua Sha, to treat soft tissue injuries by improving mobility, reducing pain, and promoting healing. These techniques can be classified as either mechanical, where tools directly apply pressure and movement, or manual, involving hand-held instruments. Unlike manual soft tissue techniques, which rely on the therapist’s hands, IASTM provides more targeted and consistent pressure, allowing deeper tissue penetration and more precise treatment for issues like scar tissue or fascial adhesions. The tools used in IASTM allow for targeted pressure, enabling practitioners to access deeper layers of fascia and muscle tissue, which can be challenging with manual techniques. This precision is enhanced by the mechanical advantage of the tools, allowing for consistent and controlled force application, which may be harder to maintain with MFR, especially on larger or denser tissue areas. It has recently emerged as an alternative tool to traditional myofascial release (MFR) techniques since the traditional MFR is administered by therapists’ hands, thereby imposing risks of overuse and arthritis of hand joints. IASTM also has an added advantage of requiring less time for treatment. IASTM is a highly effective treatment for musculoskeletal injuries, offering several advantages over traditional therapies. It enables clinicians to target deep tissue layers with precision, improving blood circulation and promoting healing by stimulating a controlled inflammatory response. This targeted approach enables the practitioner to address both superficial and deep fascial restrictions, something that manual techniques might not always reach effectively. IASTM helps break down scar tissue and fascial adhesions, reducing pain and improving range of motion more quickly than passive treatments like ice or heat. It is versatile, addressing a wide range of conditions such as tendinopathies and muscle strains, and can be combined with other therapies for enhanced results [18–20].
According to the literature, using instruments for soft tissue mobilisation increases vibration sensitivity, which makes it easier for the clinician to notice changes in the tissue’s characteristics. IASTM has garnered attention for its potential therapeutic benefits, yet it is surrounded by controversies and notable gaps in the literature. While some studies suggest its effectiveness in improving pain and range of motion, others indicate that it may not be significantly more effective than alternative therapies [19]. Although there is growing evidence on the effect of IASTM, there is no conclusive evidence yet on whether it offers significant benefits or merely results in a placebo effect [20]. Further, a review of the literature suggests a dearth in the literature regarding interventions using IASTM to release the QL and its effect on pelvic posture correction [14, 15].
The study aimed to achieve two main objectives. The first objective was to evaluate the effects of IASTM in participants with NSLBP on the length of the iliopsoas measured by diagnostic ultrasound and the Thomas test, pelvic posture, pain and disability. The second objective was to determine whether IASTM is significantly more effective than sham IASTM, with a focus on evaluating any potential placebo effect.
The findings of this study could have significant clinical implications in the treatment of NSLBP. If instrumental MFR is shown to effectively lengthen the iliopsoas and QL muscles, it could become a valuable intervention for improving pelvic posture and reducing pain and dysfunction in NSLBP participants. Furthermore, if IASTM is proven to be more effective than a placebo treatment, it could provide evidence supporting its use as a targeted therapy for soft tissue dys-function in back pain management [1, 18, 19], offering clinicians an evidence-based approach to improving patient outcomes.
Subjects and methods
Study setting and design
This research was a randomised, double-blind, placebo-controlled study conducted at the Tertiary Care Centre of Belagavi city, India, between February 2022 and January 2023.
Population and sample
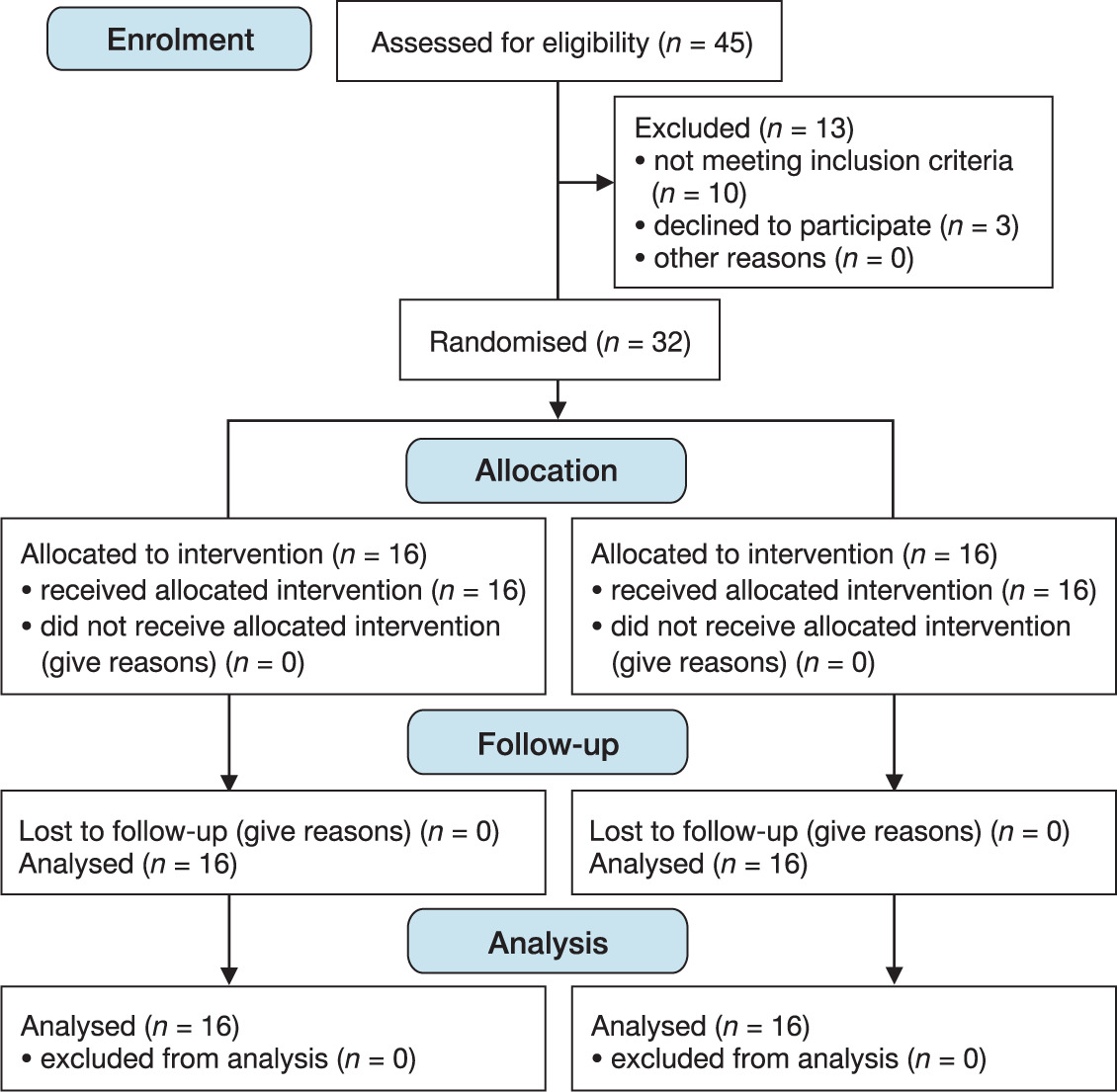
Participants were briefed on the study’s purpose and procedures before it began. Out of 45 individuals with NSLBP screened for eligibility, 32 met the pre-established criteria. The participants were randomly allocated to either the experimental or control group using a lottery method with a 1:1 ratio. The investigator responsible for delivering the intervention also handled the enrolment and allocation of participants. To enhance the reporting quality of the trial, the consolidated standard of reporting trials (CONSORT 2010) guidelines were followed, along with the Template for intervention description and replication (TiDier) checklist that aimed at assessing the quality of the intervention (Figure 1).
Selection criteria
Individuals clinically diagnosed with NSLBP by a qualified physiotherapist based on history and physical examination identification of red flags using neurological testing and imaging if serious pathology is suspected [21], in the age group of 18–60 years with a score of 3–7 on the visual analogue scale (VAS) and who present with a positive result on passive trunk rotation testing for QL tightness [3] were included. The specific intensity of the VAS score was chosen to include individuals with moderate pain, which is common in NSLBP participants. This range allows for the evaluation of treatment efficacy in individuals with clinically relevant pain, ensuring that the results can be generalised to a significant portion of the NSLBP population. Individuals who had a history of spinal surgery, or a diagnosis of lumbar spondylosis, lumbar radiculopathy, ankylosing spondylitis, or prolapsed intervertebral disc were all excluded from the study. In addition, individuals with open wounds on their back, sensitive skin, or an allergy to gel were also excluded considering the potential adverse reactions to IASTM. To minimise participant dropout, strategies such as thorough screening during the recruitment process were implemented to ensure only those meeting the inclusion criteria were selected. Furthermore, regular follow-ups were conducted throughout the study to address any concerns or discomforts promptly, helping to maintain participant engagement and reduce dropout rates. Participants were also provided with clear instructions and support to enhance their adherence to the study protocol.
Sample size calculation
Sample size was calculated as follows: n = 2 S2 (Z + Z) 2/d2, where S (standard deviation) = 3.98; Z = 1.96 at 5% d-error (significance level); Z = 0.842 at 75% power (Power); and d = 3.98 (x1–x2) effect size referring to the article with a psoas length by the modified Thomas test [13]. The sample size was calculated to be 16 in each group, which is 32 participants in total.
Interventions
The same conventional physiotherapy was given to both groups by a qualified and trained physiotherapist. The intervention was an individualised approach in the form of a common protocol applied to both groups, with all treatment sessions provided face-to-face in an outpatient physiotherapy department of a tertiary care hospital. To minimise dropouts during the study, strategies such as regular follow-up reminders and flexible scheduling were employed to maintain participant engagement. No loss to follow-up was reported, and all the participants completed the intervention protocol.
Treatment included
Interferential therapy (IFT) was administered using a VECTROSTIM-100 5-in-1 computerised machine (Bionix, Mumbai, Maharashtra), equipped with four electrodes (10 × 12 cm, 75 cm2) arranged in a crossed pattern over the 1st and 5th lumbar vertebrae. Treatment parameters included a 4 kHz carrier frequency, 65 Hz amplitude modulated frequency, and 95 Hz sweep frequency with a 1:1 swing pattern. A triangle approach was used, and the intensity was adjusted to the patient’s tolerance. Participants were informed to expect a ‘pins-and-needles’ sensation and instructed to report any unusual sensations. The therapy session lasted 25 min to facilitate pain relief [22].
Therapeutic ultrasound (Bionix, Mumbai, Maharashtra) of 1-MHz frequency, continuous mode, with an intensity of 1 W/cm2 and a treatment head area of 5 cm2 was selected. This was given for 5 min at the lumbar region around the paraspinal area where the most pain was felt by the patient [22].
IASTM/experimental group (group 1)
The subject was positioned prone, lying with the lower back area exposed. An IASTM tool (Modified – Graston®) was used to release the QL muscle by applying petroleum jelly to avoid friction. Strokes were given in the direction from the posterior border of the iliac crest to the inferior border of the 12th rib and the L1–L4 to release the QL bilaterally with a pressure of 250 gm/cm2, which the treating physiotherapist practiced beforehand on a weighing scale retrospective to the treatment [23]. Five sessions of IASTM were given every alternate day followed by cryotherapy for 10 min (Figure 2). Cryo-therapy was given to reduce the inflammation that may be caused following myofascial release, and to address post-treatment soreness.

Sham/control group (group 2)
The common intervention along with sham IASTM release was given to the control group. While administering the sham IASTM, negligible pressure was applied on the skin, during which the physical aspects of the technique were stimulated without delivering its therapeutic effects. IASTM was given in the same motion or technique as in the experimental group but avoided applying sufficient force to stimulate the tissue. This approach ensures that any changes in the participants’ condition are likely due to psychological factors, such as the placebo effect, rather than the actual therapeutic impact of IASTM.
Selected participants with NSLBP were asked to visit the outpatient department (OPD) setting every alternate day for 5 sessions across 10 days. The treatment lasted from 45 min to 1 hour.
Outcomes
Outcomes measures were assessed twice, i.e. on day 0 (pre-treatment) and on day 10 (post-treatment). Diagnostic ultrasonography was conducted by a qualified radiologist, while a qualified physiotherapist assessed the other outcomes. Both of these assessors were blinded to the participants’ group allocations. The blinding was maintained in two ways: First, the diagnostic USG was performed by a radiologist who was unaware of the participants’ group assignments. Second, the clinical assessments, including the Thomas test and other evaluations, were conducted by a qualified physiotherapist who was also blinded to the intervention given to the participants. To further ensure blinding, participants’ identities were coded, preventing any sharing of personal information that could reveal group allocation.
Primary outcomes
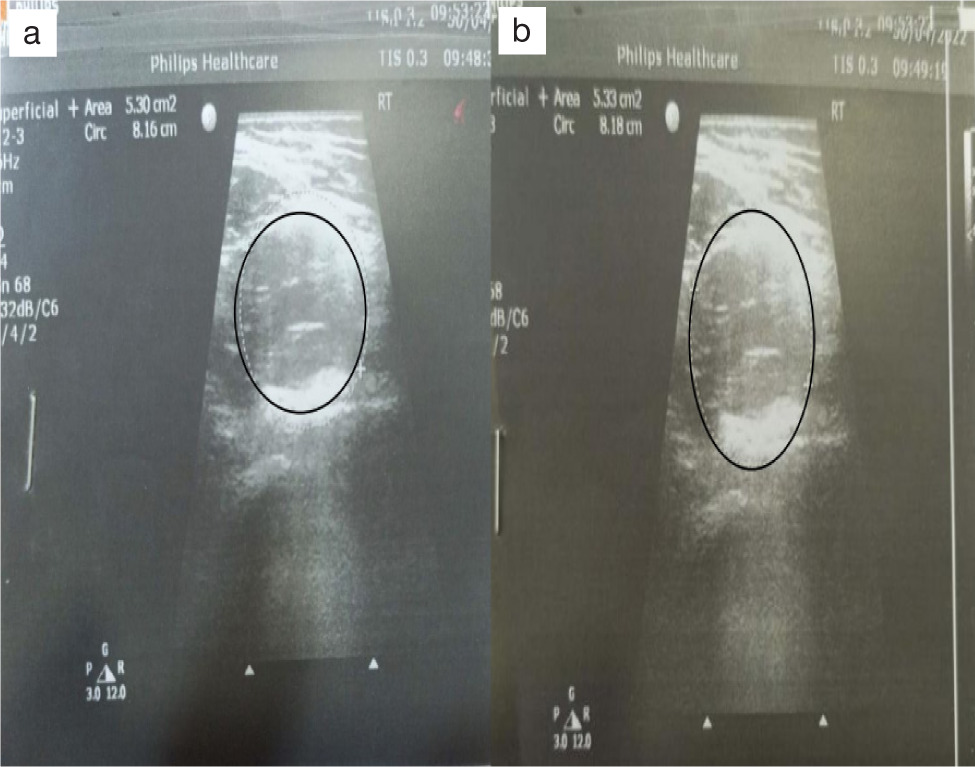
Iliopsoas muscle length using diagnostic USG: The assessment of iliopsoas length was performed by a qualified radiologist. Muscle length was measured in millimetres using a portable real-time ultrasound unit with a curved linear array transducer of 4 MHz and a water-soluble transmission gel. The imaging of the iliopsoas muscle was conducted by placing the transducer directly over the hip joint on the inguinal crease. The image boundaries were defined using landmarks like a visible crescent of echogenic brightness for the anterior femoral head and the pulsing femoral artery. For capturing images of the anterior thigh, the transducer was positioned at the level of the greater trochanter. Each muscle was imaged twice on both sides, with the probe lifted off the skin between each image [24]. For the USG, both the intra-rater reliability and inter-rater reliability interclass correlation coefficient (ICC) (2, 2) were higher for psoas muscle length [25] (Figure 3).
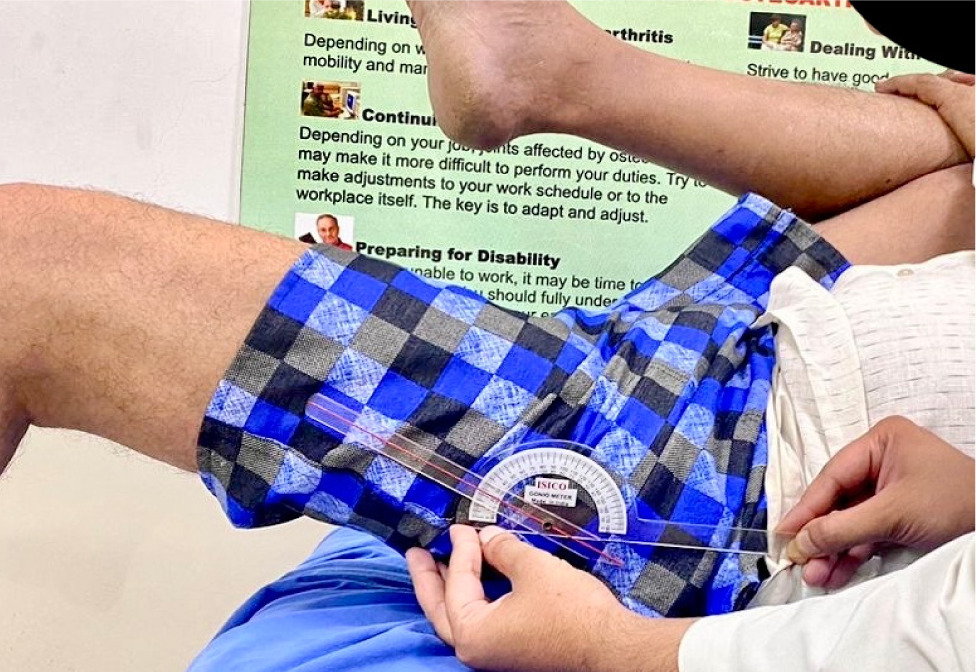
Modified Thomas test to check the length of the iliopsoas muscle: The participant flexed and pulled the non-test limb towards their chest while sitting on the edge of the table or couch with the lower limb that would be tested off the surface. The hip flexion range was assessed using a universal goniometer, with the movable arm aligned with the lateral aspect of the femur, the stationary arm parallel to the couch, and the fulcrum on the greater trochanter. Pre- and post-intervention bilateral measurements were taken, and the results were reported in degrees [3]. The ICC value for the goniometric measurement of the modified Thomas test was 0.92, suggesting high reliability [26] (Figure 4).
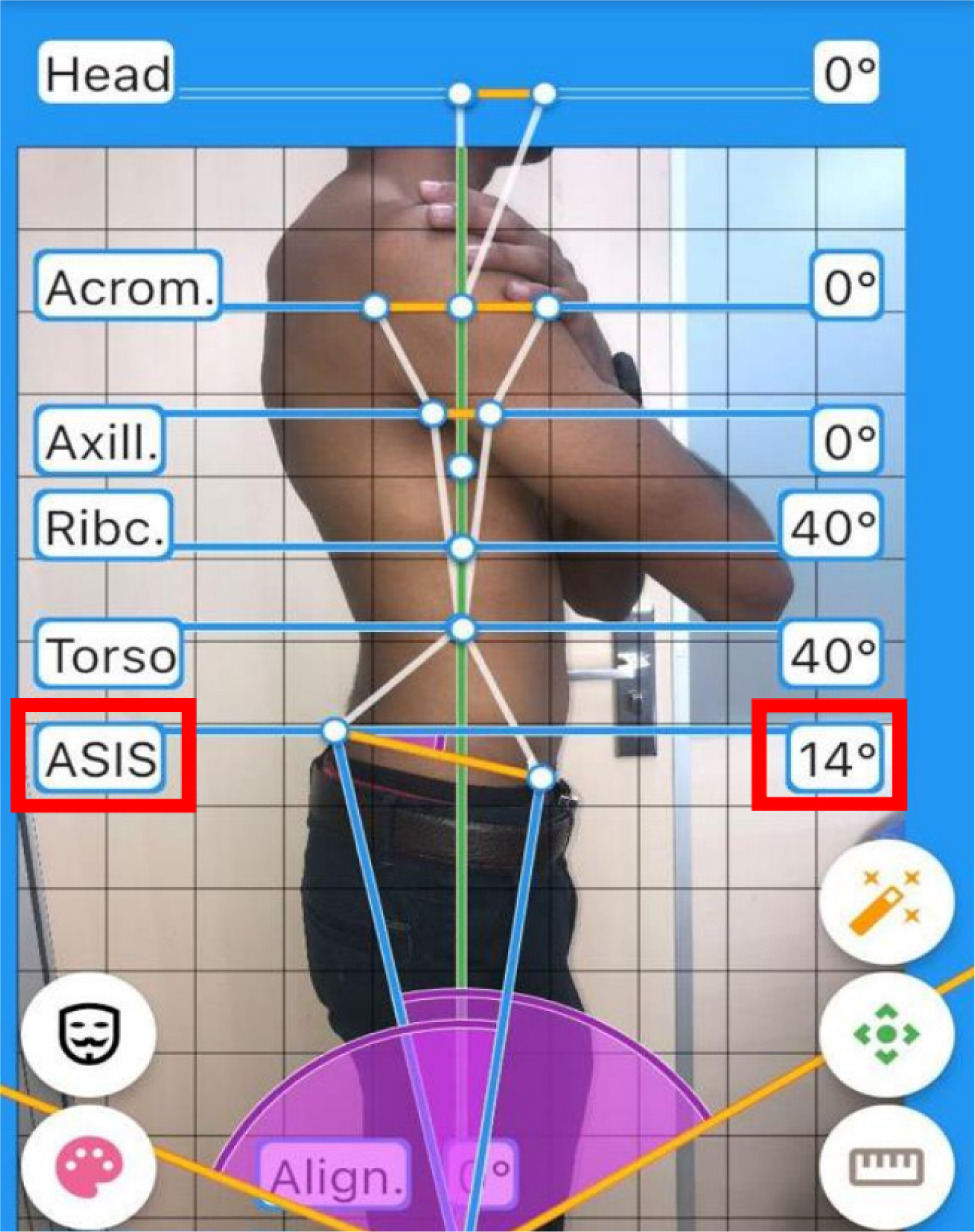
Assessment of pelvic posture by APECS software application: This is an artificial intelligence-based assessment for anterior pelvic tilt where the participant stands on a flat surface, dressed in minimal, form-fitting clothing. A lateral photo was taken while they stood still with their hands crossed over the chest and the feet spaced equally apart. The anterior and posterior-superior iliac spines were palpated and marked with adhesive glow tape. A camera mounted on a tripod 1.5 m away captured the image from the right side to quantify the anterior pelvic tilt [27]. The Pearson correlation coefficient between the APECS application and the gold standard (X-ray) was 0.9874 (98.74% of matching). The agreement between standard radiograph, and the average of all examiners’ APECS Pro measurements (including right and left sides) equalled 94.64% (kappa = 0.8323; p = 0.001), which suggests very good agreement [28] (Figure 5).
Secondary outcomes
Quebec back pain disability scale (QBPDS): The QBPDS was selected over other back disability scales due to its high sensitivity in assessing LBP, making it particularly suitable for evaluating functional limitations and pain in individuals with long-term conditions. There are 20 items in this questionnaire that are related to activities of daily living, it is self-administered and uses a 6-point scale between 0 (not difficult) and 5 (unable to perform) with a total score ranging between 0 and 100 and an inter-rater reliability of 0.90. Participants who did not understand English were provided with a translated version in their native language [29].
Visual analogue scale (VAS): This is an objective, established scale for measuring both acute and ongoing pain. Scores were recorded by handwriting a mark on a 10-centimetre line that corresponds to a continuum between ‘0’ for no pain, ‘1–3’ for light discomfort, ‘4–6’ for moderate-to-severe pain, ‘7–9’ for very severe pain, and ‘10’ for the worst agony [30]. Both the intra-rater VAS reliability (Cronbach’s alpha: 0.951, ICC: 0.951, 95% CI: 0.916–0.971, p < 0.001) and inter-rater VAS reliability (Cronbach’s alpha: 0.959, ICC: 0.959, 95% CI: 0.929–0.976, p < 0.001) were very high [31].
Statistical analysis
Data collected was tabulated and analysed for statistics using Statistical Package for the Social Sciences (SPSS) version 23.0. For handling missing data, statistical methods such as multiple imputation were used to account for incomplete responses, minimising bias and preserving the study’s integrity by including all participants in the analysis, regardless of whether they completed all aspects of the study. For categorical data, a frequency analysis was performed, while for continues variables, the mean and standard deviation or median and interquartile range (IQR) were analysed. Data was analysed for normality using the Kolmogorov–Smirnov test, which showed the data was not normally distributed. Hence, the within-group analysis was performed using the Wilcoxon matched-pairs test, and the between-groups analysis was performed using the Mann–Whitney U test. The probability value for statistical significance was set at p < 0.05.
Results
Descriptive statistics
The participant’s demographic features in both groups show no significant differences, indicating a normal distribution of participants (Table 1). Regarding the gender, the number and percentage of male and female participants in the IASTM group were (male: n = 9; 56.25% and female: n = 7; 43.75%) and sham IASTM group were (male: n = 8; 50.0% and female: n = 8; 50.0%).
Table 1
Demographic characteristics#
Inferential statistics
Within-group analysis
In the IASTM group, the results showed that the % change from pre to post for the length of the right iliopsoas using USG was −2.95% (effect size 0.76) and for the left iliopsoas was −3.79% (effect size 0.81). The modified Thomas test angle % change on the right side was 15.52% (effect size 0.78), while for the left, it was 15.41% (effect size 0.80). The anterior pelvic tilt % change was 13.17% (effect size 1.07), while for the VAS and Quebec back pain disability, the % change was 46.31% and 48.16% (effect size 1.47 and effect size 1.44), respectively. The p-values for all the outcomes in the IASTM group were statistically significant with p < 0.001 (Table 2).
Table 2
Within-group comparison for experimental/IASTM group
The % of change for the within-group analysis from pre to post in the Sham IASTM group for the length of the right iliopsoas using USG was −0.17% (effect size 0.03) and for the left, −0.08% (effect size 0.06). The Modified Thomas test angle % change observed on the right was 3.60% (effect size 0.34) and for left, it was noted to be 2.91% (effect size 0.50), followed by the anterior pelvic tilt % change being 1.59% (effect size 0.22). The VAS and Quebec back pain disability showed % changes of 43.80% and 46.91% (effect sizes 1.63 and 1.42), respectively. Only the VAS and Quebec back pain disability showed statistically significant changes with p < 0.05. However, all the other outcomes were statistically insignificant changes (p > 0.05) (Table 3).
Table 3
Within-group comparison for control/sham IASTM group
In the IASTM group, the analysis proved to be superior in terms of the increase in the length of the iliopsoas and the reduction in the modified Thomas test angle and anterior pelvic tilt. The VAS and Quebec back pain disability were proven to show similar results in both the groups.
The between-groups analysis using the Mann–Whitney U test revealed that the iliopsoas muscle length and modified Thomas test angle improved significantly more in the IASTM group compared to the control group, with a p-value of 0.0001 (Table 4). As shown in Table 5, the p-value for the between- -groups analysis of the Quebec back pain disability score was 0.83, which is more than the pre-set significance value, hence inferring that no significant change was seen in the IASTM/experimental group when compared to the sham/control group. The p-value for anterior pelvic tilt was 0.0001, which means that the IASTM group was better than the sham/ control group. The VAS scores in the IASTM group were slightly better than the control group, with a p-value of 0.04 (Table 5).
Table 4
Between-groups analysis using Mann–Whitney U test for length of iliopsoas and modified Thomas test
Table 5
Between-groups analysis using Mann–Whitney U test for anterior pelvic tilt, VAS and Quebec back pain disability score
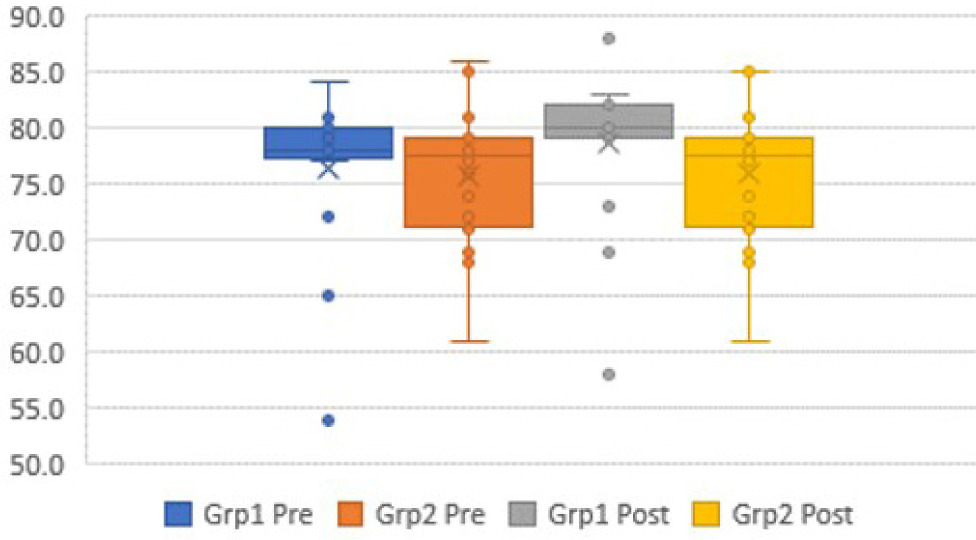
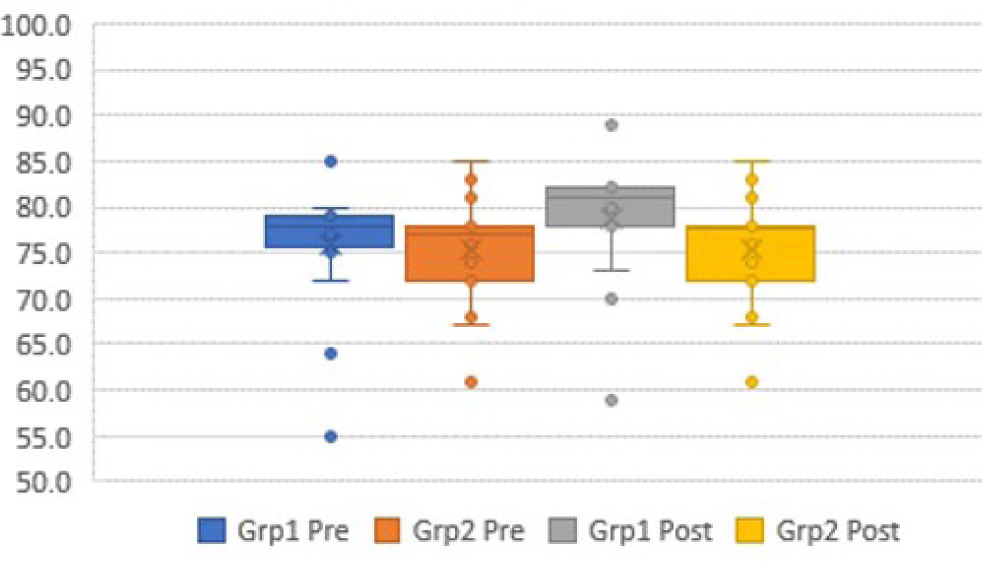
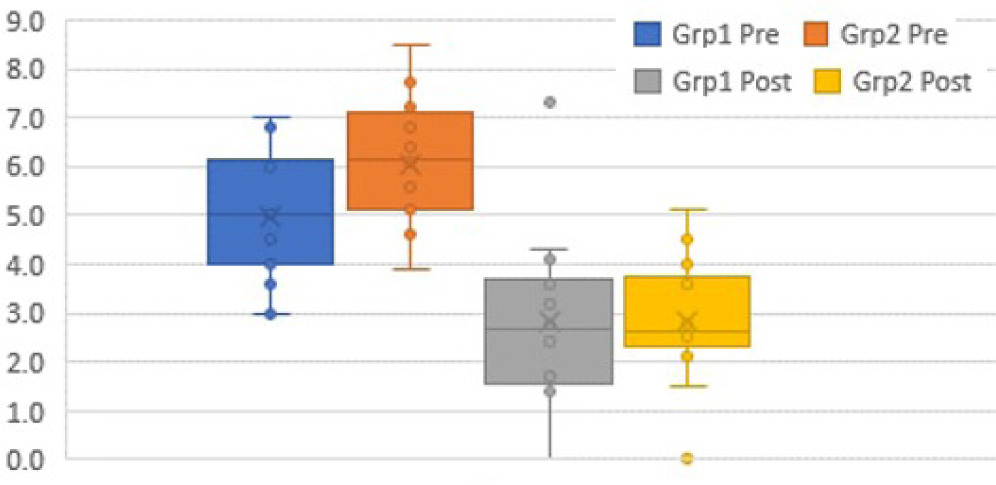
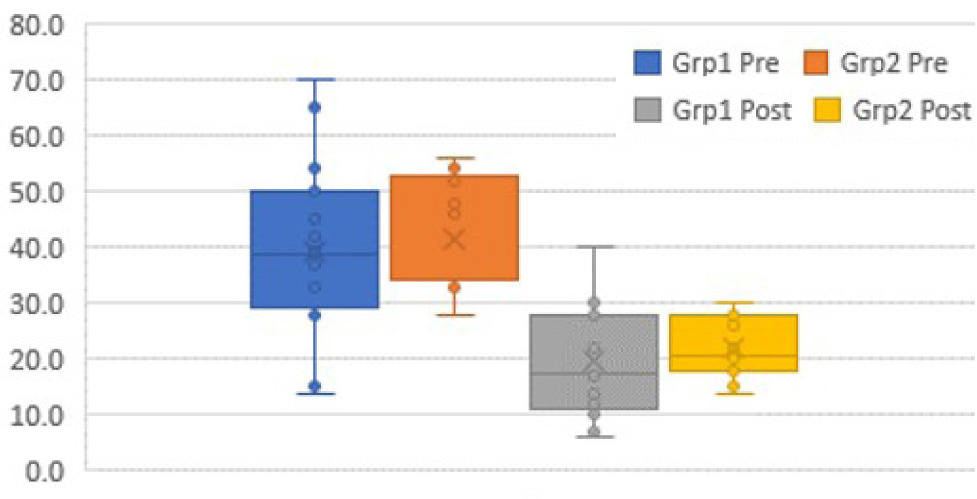
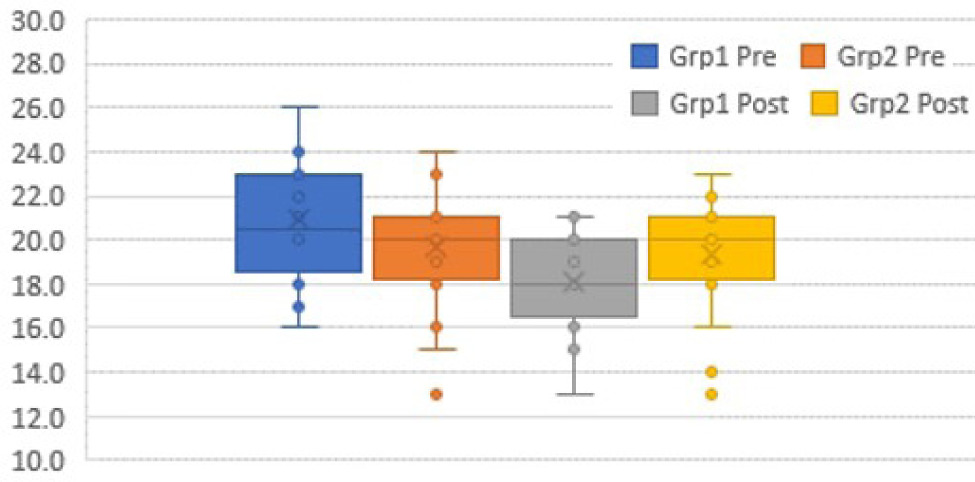
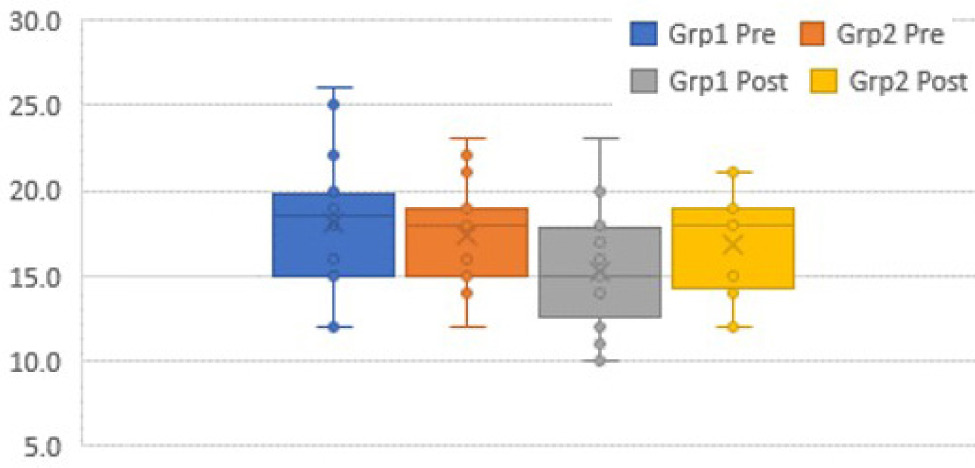
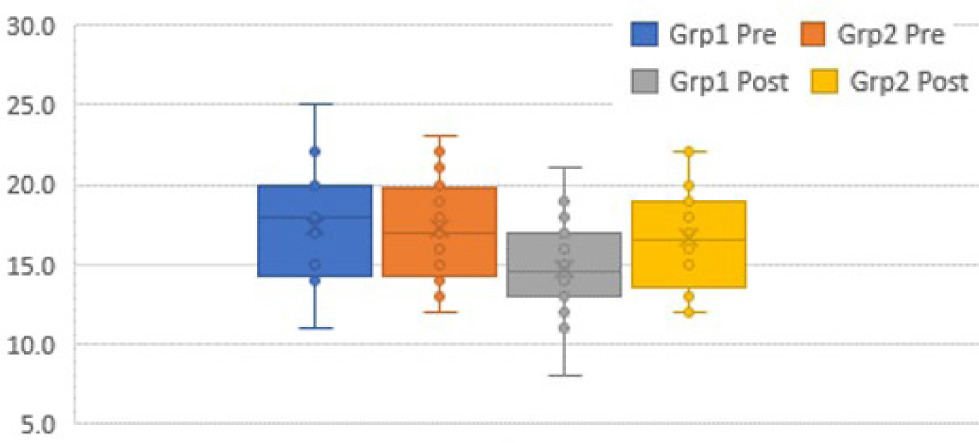
The box plots (Figures 6–12) provide a pictorial depiction of all outcomes between the groups.
Discussion
Since the experimental group showed better outcomes than the control group, the alternative hypothesis was accepted. IASTM release was more effective in increasing the length of the iliopsoas, reducing the Modified Thomas test angle, and improving pelvic posture in the intervention group. In contrast, the control group showed greater pain reduction. The aim of this study was to evaluate the effects of IASTM release on the quadratus lumborum (QL) and its impact on iliopsoas length, pelvic posture correction, the Modified Thomas test as test angle, pain, and quality of life (QOL) in individuals with nonspecific chronic LBP.
The results revealed equally significant improvements in QOL and a reduction in pain severity for both groups. Specific data showed that the experimental group experienced an increase in iliopsoas length [right iliopsoas −2.95% (p-value 0.0004), and left iliopsoas −3.79% (p-value 0.0004)] with no changes in the control group.
The current study demonstrated a significant increase in the iliopsoas length with IASTM for the quadratus lumborum. Firstly, it could be because of the anatomical connection of common insertion, and secondly, this could be due to the presence of the deep sheath of thoracolumbar fascia that divides the two muscles, placing the iliopsoas deeper than the QL, and hence making it difficult to directly target the iliopsoas. Thirdly, it is due to the continuous myofascial connection and similar insertion of these two muscles. This aligns with another study that found IASTM led to observable morphological changes in tissues, confirmed through ultrasound examination. These changes directly indicated musculoskeletal functional recovery and have been shown to improve LEFS scores [23]. Hence, targeting the QL would be an effective and more feasible method of management instead of attempting to target deep-situated muscle.
The current study demonstrated a correction in pelvic tilt following IASTM to the tight QL muscle. It is stated in the literature that releasing the tight QL has an indirect effect on pelvic posture by improving the length of the surrounding hip and knee muscles [13]. The QL activity plays a crucial role in pelvic motor control in the coronal plane. Improving QL function is vital for correcting lumbopelvic alignment, as there is a positive correlation between QL activity and changes in pelvic tilt angle. The findings of Oshikawa et al. [12] provide the foundation for the results observed in the current study.
Similarly, previous studies have reported that IASTM (Graston Technique®) effectively enhances hip joint flexibility in participants with chronic LBP compared to static stretching, aligning with the results of the current research [32, 33]. However, one of the previous studies conducted was able to demonstrate an immediate change in muscle function despite only a single application of IASTM [32], while the present study delivered 5 sessions of IASTM on the QL. Therefore, a significant difference was observed in the intervention group on the pelvic posture as QL and iliopsoas tightness are both associated with anterior pelvic tilt. The five IASTM sessions in the present study allowed for cumulative effects, leading to more significant and lasting improvements, particularly in pelvic posture, leading to more noticeable corrections in pelvic posture compared to a single application.
The stretching of the quadratus lumborum (QL) muscle plays a significant role in managing LBP, particularly in cases of non-specific pain and myofascial pain syndrome. In line with the findings of the present study, previous research indicates that passive stretching and myofascial release of the QL can effectively reduce pain and improve functional outcomes in participants suffering from LBP [34]. A study demonstrated that a combination of myofascial release, muscle energy techniques, and QL stretching led to significant improvements in pain and lumbar range of motion [35]. Research comparing passive stretching to post-isometric relaxation techniques showed that both methods effectively reduced pain intensity, with passive stretching being beneficial for trigger points in the QL [34]. The QL is often a site for myofascial trigger points, which can exacerbate LBP. Effective palpation and treatment of these points through stretching and manual techniques can alleviate symptoms [36, 37]. Incorporating stretching into a broader treatment plan, including posture correction and ergonomic adjustments, can enhance recovery outcomes for participants with chronic LBP [36].
The application of IASTM offers several comparative advantages over manual techniques like passive stretching, myofascial release, and manual mobilisation techniques for managing LBP. These advantages include enhanced pain relief, improved range of motion, and greater functional outcomes due to targeted release of fascia and reduced hand fatigue for therapists [38]. However, a systematic review conducted on the effects of instrument-assisted soft tissue mobilisation compared to other manual interventions like stretching, MFR etc. on pain and function concluded that IASTM had a positive short-term impact on the functionality of individuals with soft tissue dysfunctions [39]. However, comparative trials are lacking where long-term effects of IASTM have been studied with prospective or follow-up studies to understand its carryover effects.
In the current study, it was found that there was no significant difference between the intervention and placebo groups with respect to the QBPDS or VAS score, indicating an equal effect between both groups. One possible reason for this is that both groups received a common intervention in the form of electrotherapy modalities, which work to reduce pain and spasms. This indicates the changes were observed only in the subjective outcome variables in the sham control group, while the experimental group showed changes both in objective as well as subjective outcomes. There is supporting evidence that evaluated the effect of back school exercises in the Chinese population with LBA on various mobility and disability outcomes [40]. Another study conducted a review on mobilisation for LBA on different outcomes of pain and functional disability, with the study concluding significant improvements in the outcomes that are similar to the findings of the present study [41].
IASTM is effective in addressing LBP by targeting soft tissue restrictions, promoting fascial remodelling, and improving blood flow, which together reduce pain. In the context of pelvic tilt biomechanics within a closed kinematic chain, IASTM helps correct dysfunctional pelvic positioning such as an anterior or posterior pelvic tilt by releasing tight muscles like the quadratus lumborum, as conducted in the current research [38]. These adjustments to muscle tension and tissue flexibility can alleviate strain on the lumbar spine. IASTM can help release muscle tightness, restore proper alignment, and reduce compensatory patterns, ultimately improving overall pelvic mechanics and reducing chronic LBP [38, 39].
The strength of the study is that it compared the role of IASTM along with the placebo control group in order to explore and prove the efficacy of IASTM. We also targeted the commonly overlooked muscular cause of LBP, which is a tight QL, and its effects on posture were analysed. Most studies on LBP management typically focus on muscles like the erector spinae, multifidus, or hip flexors, which are commonly associated with lumbar instability and pain. These approaches often emphasise strengthening or stretching these muscles. However, the present study uniquely targets the quadratus lumborum (QL), a deep muscle that plays a crucial role in maintaining pelvic stability and posture. Tightness in the QL is strongly associated with conditions like anterior pelvic tilt, which contributes to LBP. By focusing on the QL, this study highlights a less commonly addressed muscle, offering a potentially more effective strategy for correcting postural imbalances and relieving chronic LBP. This approach is distinct in its emphasis on releasing QL tightness to improve both muscle length and pelvic posture. A quantitative outcome in the form of ultrasonography measures was taken as the primary outcome for assessing the length of the iliopsoas.
Limitations
There were a few limitations. A wide range of ages (18–60 years) was included in the study, but the participants involved in the study were not distributed equally across the given age range. The outcomes were not compared between sexes for differences and were not analysed based on their BMI classification. The sole effect of IASTM release on pain could not be observed because a pain-relieving modality was given to both groups. Also, there was a lack of post-treatment follow-up.
Conclusions
In conclusion, only IASTM, and not sham IASTM, significantly reduced anterior pelvic tilt and increased iliopsoas length. Therefore, IASTM is an effective technique for soft tissue release and correcting tight structures. Additionally, releasing the QL can lead to the release of a tight iliopsoas, which in turn affects pelvic posture. Thus, QL release should be considered for participants with LBP to help correct pelvic posture and target the deep-seated iliopsoas muscle.
Clinical implications
This study demonstrates that IASTM effectively reduces anterior pelvic tilt and increases iliopsoas length, making it a valuable tool for soft tissue release and addressing tight structures. Integrating IASTM into rehabilitation protocols allows clinicians to release muscle tightness, improve muscle length, and restore proper pelvic alignment, which can help alleviate pain and enhance mobility in individuals with chronic LBP. To optimise rehabilitation for chronic nonspecific LBP, incorporating IASTM to target soft tissue restrictions and improve pelvic posture, along with QL release techniques to address the deep-seated iliopsoas, provides a comprehensive approach. This combined strategy offers a more holistic and effective treatment option for individuals experiencing chronic LBP.