Introduction
An individual’s hands are extremely significant for good reasons. Many corresponding activities are accomplished by hand in conjunction with human transmission, device care, and various other activities of daily living [1]. Grip strength is evaluated by assessing the total static force produced by the hand using a dynamometer and pinch meter, in kilograms (kg) or pounds. It is also measured in millimetres of mercury and newtons [2]. Handgrip strength is one of the major elements affecting muscle performance, which must be ensured in any upper extremity rehabilitation program [3]. Over the years, several instruments for measuring handgrip and pinch strength have been developed. In 1950, instruments like the Sklar, Narragansett, Geckler, and Collins dynamometers were developed, which had a few limitations for assessing accurate grip strength assessment [4]. In 1954, Bechtol developed the Jamar dynamometer. It proved to be the best instrument for handgrip strength measurement [5]. Then, in 1958, Brewer et al. introduced the sphygmomanometer to measure hand-grip strength. Based on the pneumatic, spray, and hydraulic systems, they concluded that the Jamar dynamometer produces accurate measurements [6]. As stated by the American Society of Hand Therapists, the Jamar dynamometer and pinch meter are the gold standard instruments for measuring handgrip and pinch strength [7]. In 2015, Hogrel [8] reported that the Jamar dynamometer may not be a convenient tool for some individuals and may also lead to hand pain because of its narrow contact area. Also, one undeniable possibility is that grip strength and pinch strength recording using a Jamar dynamometer and pinch meter, correspondingly, can be done manually (i.e. which can introduce man-made bias) in clinical practice. Recently, in addition to the gold standard instruments, several studies have reported the comparison of newly designed instruments to prove their efficacy, validity, and reliability in measuring the hand-grip strength and pinch strength, such as the electronic dynamometer (2011), MyoGrip and integrated digital dynamometer (2015), computerised digital dynamometer (2020), and digital pinch meter (2012, 2019). However, none of them are dual purpose as they measure handgrip strength and pinch strength using two different instruments. They need the supervision of an expert and do not even contain data logging features or real-time statistical analysis. Also, they are not easily available except in hospitals, research centres, and medical institutes due to their high price. Therefore, there is a need to develop an electronic dynamometer with automatic grip strength data recording, which will be cost-effective and, most importantly, comfortable and convenient to use for all individuals. The device facilitates recording the data digitally for further statistical analysis and research purposes as it is connected to a smartphone via Bluetooth, which contains a mobile application that stores all the data permanently, among other tasks. Therefore, the objective of the study was to develop an electronic dynamometer to measure the hand-grip strength and pinch strength, to determine the validity of the Bluetooth-enabled smart hand dynamometer (BESHD) for calculating the handgrip strength and pinch strength, and to calculate the intra-rater reliability of the BESHD for measuring the handgrip strength and pinch strength.
Subjects and methods
Study design
It was a cross-sectional observational study that was conducted at the Tertiary Care Hospital of the Dr. D. Y. Patil Hospital & Research Centre, Pune, India.
Participants
The participants were young, healthy individuals. They were selected using a convenient sampling method. Participants who were willing to participate, in the age range of 22 to 40 years, and both men and women met the inclusion criteria. The exclusion criteria were participants having any upper extremity disorder, those who had undergone recent hand surgery in the past 6 months, and those with ambi-dexterity. Initially, permission for the construction of the new electronic handgrip device along with the software application for recording the individual’s data was granted by the Engineering and Technology Department. After the construction of the device and application, an initial pilot study was conducted on 10 participants to determine the validity and reliability of the newly designed electronic dynamometer. Participants aged 22 to 40 years were divided into 2 groups: group A (5 per group) and group B (5 per group). Participants aged 22 to 30 years were included in group A while group B included the participants aged 31 to 40 years. In group A, hand grip strength and pinch strength were determined using a pinch meter and a Jamar dynamometer, then the BESHD was applied. Similarly, in group B, the same were measured with the BESHD followed by a Jamar dynamometer and pinch meter with a 3–5 min break in between. Three trials were undertaken with a 1–min break in between each trial, by the same therapist, and the maximum reading was considered as the final reading. The durations of the trials and rest periods was recorded using a stopwatch. Based on the results obtained, the sample size was calculated. The main study was carried out on 110 participants in a similar manner as the pilot study.
Instrumentation
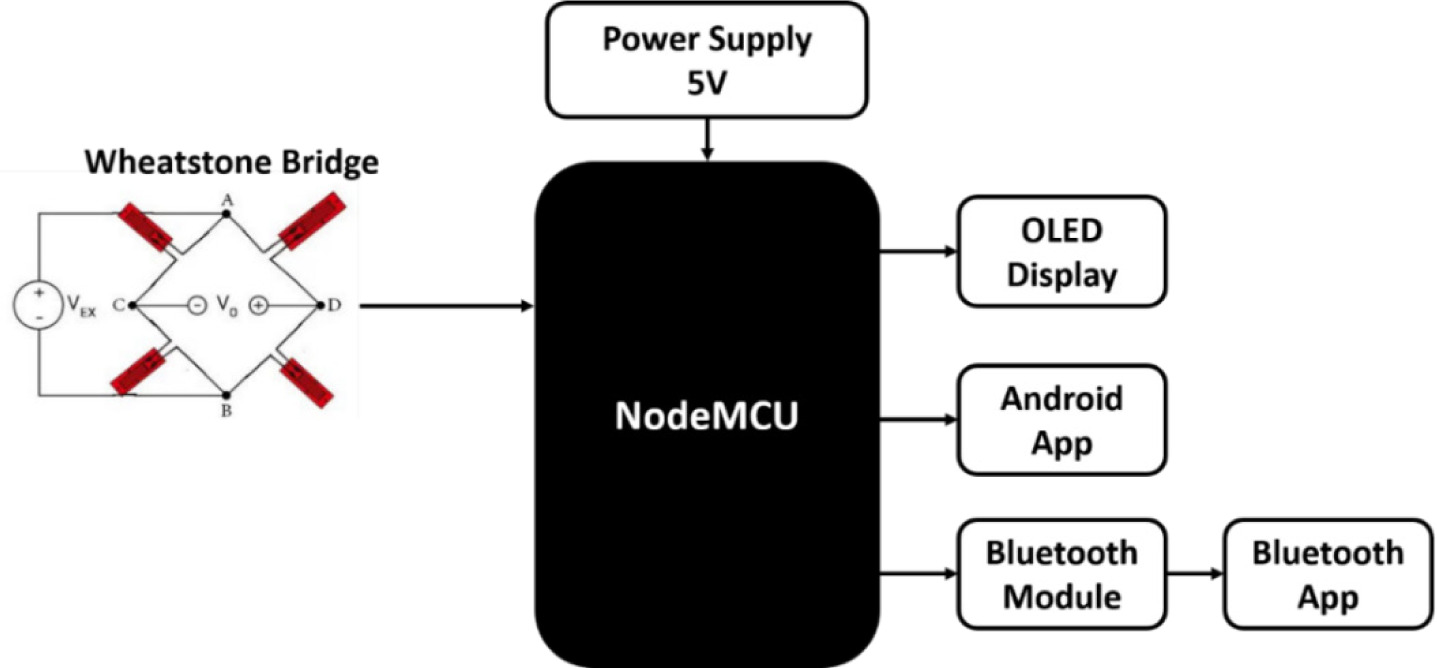
The suggested framework, as shown in Figure 1, accepts input from FlexiForce A301-100 force sensors. The sensor provides an analogue value. The NodeMCU has only one analogue PIN, which is why a Wheatstone bridge circuit was used to select input from each sensor. The sensor value is measured in terms of the load received by the sensor. Estimated values are displayed on the OLED display. A Blue-tooth app was designed to display readings on an Android phone. To send sensor data to the mobile app, a HC05 Blue-tooth module is connected to the NodeMCU board. The user then connects the device to the smartphone via the HC05.
Procedure for calibration / construct validity of device
(A) Procedure – The device is a designed sensor interfaced with an electronic circuit. The sensor was placed on a weighing machine. The force was applied by a finger on both sensors, which in turn also applied this force to the weighing machine. The weights shown on the weighing machine and the device’s display were compared for confirmation. The detailed calibration report is shown in Table 1.
(B) Calibration report (Table 1).
Study procedure
The Jamar dynamometer, pinch meter, and BESHD were used to test the participants’ grip and pinch strengths. The strength of the pinch and handgrip were assessed on each hand with the Jamar dynamometer and pinch meter as detailed in the guidelines of the American Society of Hand Therapists. The measurements were also taken using the Blue-tooth-enabled smart hand dynamometer.
Subject position
Subjects were put in a sitting position on a chair with their back straight, using a footrest, hips and knees at approximately 90°, elbow of the arm under test at rest at approximately 90°, shoulder in adduction, and elbow flexion at approximately 90° to 120°. The forearm and wrist were placed neutrally between 0 and 30° extension, and 0 and 15° ulnar deviations. Three trials were conducted for both the dominant and non-dominant hands on the BESHD and Jamar dynamometer as well as the pinch meter with 1 min of rest in between the trials and 3–5 min of break in between each piece of measuring equipment. The maximum reading was considered the best score.
Procedure for calculating maximum voluntary contraction with Jamar dynamometer
The Jamar dynamometer was held keeping all fingers on the grip band, placing the index finger at the top of the grip. The second dynamometer handle position was used. Subjects were instructed to exhale while gripping the dynamometer and holding it for 5 s along with 1 min of rest between the repetitions. The grip strength was assessed for the dominant hand followed by the non-dominant. Both hands were assessed alternately. The maximum score among the three repetitions was considered as the handgrip strength.
Procedure for calculating maximum voluntary contraction with BESHD
After measuring the maximum handgrip strength with the Jamar dynamometer, the same procedure was carried out with the BESHD as for the Jamar dynamometer. The dynamometer was held in the subject’s hand. The grip strength was assessed with the dominant followed by the non-dominant hand. Both hands were assessed alternately. The subject was asked to compress the entire unit as much as possible along with 1 min of rest between the repetitions. Three repetitions were taken, and the maximum score among the three repetitions was considered the handgrip strength.
Procedure for calculating pinch strength (pulp-to-pulp) with pinch meter
The pinch meter was placed between the pulp of the subject’s thumb and the pulp of their index finger and middle fingers. The subject was instructed to pinch as hard as possible. The grip strength was assessed with the dominant followed by the non-dominant hand along with 1 min of rest between the repetitions. Each finger was assessed alternately. Three repetitions were taken, and the maximum score among the three repetitions was considered the pinch strength.
Procedure for calculating pinch strength (pulp-to-pulp) with BESHD
After assessing the maximum pinch strength with the pinch meter, the same procedure was carried out with the BESHD as for the pinch meter. The subject was requested to position the fingers on the respective buttons and compress the entire unit. The subject was asked to use maximum force to compress the finger buttons of the dynamometer separately. The grip strength was assessed with the dominant followed by the non-dominant hand along with 1 min of rest between the repetitions. Three repetitions were taken, and the maximum score among the three repetitions was considered the pinch strength.
Statistical analysis
The mean and standard deviation of age were calculated. Validity was confirmed by the Bland-Altman plot method, which showed agreement between both dynamometers. Intra-rater reliability was confirmed by the intra-class correlation coefficient. The analysis was done using the MedCalc software version 20.027.
Results
The comparison of the hand grip strength measurements of the dominant and non-dominant hands between the BESHD and Jamar dynamometer is presented in Table 2.
Table 2
Comparison of measurements of dominant and non-dominant hand grip strength between BESHD and Jamar dynamometer
The difference in mean (SD) hand grip strength was significant between the dominant hand [0.54 (1.74)] and non-dominant hand [0.03 (2.12)] comparing the Jamar dynamometer and BESHD.
The comparison of the pinch strength (I–IV finger) measurements of the dominant hand between the BESHD and pinch meter is presented in Table 3. The mean (SD) difference of the pinch strength of the index finger (I) was −0.42 (1.38), middle finger (II) was −0.64 (1.83), ring finger (III) was −0.23 (1.73), of little finger (IV) was −0.81 (1.47).
Table 3
Comparison of measurements of dominant pinch grip strength (I–IV finger) between BESHD and pinch meter
The comparison of the pinch grip strength (I–IV finger) measurements of the non-dominant hand between the BESHD and pinch meter is presented in Table 4. The mean (SD) difference of the pinch strength of the index finger (I) was significant at 0.40 (1.72), middle finger (II) was −0.09 (1.75), ring finger (III) was −1.17 (1.84) and little finger (IV) was −2.25 (1.55).
Table 4
Comparison of measurements of non-dominant pinch grip strength (I–IV finger) between BESHD and pinch meter
The ICC determined the intra-rater reliability of the BESHD (Table 5). The values for handgrip strength were 0.9047 and 0.8614 for the dominant and non-dominant hand, respectively.
Table 5
Intra-rater reliability of BESHD
The values for the pinch grip strength of the I–IV fingers in the dominant and non-dominant hand ranged from 0.7247 to 0.8872.
Discussion
The current study determined the validity and intra-rater reliability of the BESHD, which is dual purpose, portable, Bluetooth-enabled, compact and contains data logging features for statistical analysis and research purposes. It measures handgrip and pinch strength. Bland-Altman plots show the comparison of measurements of handgrip strength between the Jamar dynamometer and the BESHD in the dominant and non-dominant hands. The study also compared measurements of the pinch strength of the index finger, middle finger, ring finger, and little finger between the pinch meter and BESHD in the dominant and non-dominant hands. The Jamar dynamometer showed higher hand grip strength than the BESHD in the dominant hand, whereas the BESHD showed similar hand grip strength as the Jamar dynamometer in the non-dominant hand. The BESHD showed higher pinch strength for all the fingers as compared to the pinch meter in the dominant hand. When comparing the non-dominant hand, the pinch meter showed higher pinch strength in the index finger, whereas the BESHD showed higher pinch strength in the middle finger, ring finger and little finger. Various reasons might have led to this occurrence with different physical settings of the dynamometers, length of the muscle, and position of the hand while performing the evaluations, as well as the anthropometric measurements of the participants. Based on the standard testing position of the participants using the Jamar dynamometer, it was observed that the force was applied by the middle phalanx of the fingers to produce maximal handgrip strength, whereas, when using the BESHD, force was applied mainly through the distal phalanx of the fingers to produce maximum handgrip strength and pinch strength, which showed relative variations in measurements; findings that are similar to those of previous studies [9]. According to the Koo and Li classification of the intra-class correlation coefficient (ICC), the BESHD shows good reliability in measuring the handgrip strength in both the dominant and non-dominant hands, pinch strength of the index finger, middle finger, and ring finger in the dominant and non-dominant hands, and moderate reliability of the little finger in the dominant and non-dominant hand. Variations are possible in the above findings, including for the following reasons: observation of the therapist, position of the patient, and position of holding the dynamometers. Manoharan et al. [10] reported that grip strength reduces with growing age or disability, which ultimately influences the health-related quality of life. Various factors influencing the grip strength, such as body mass index (BMI), height, weight, age, sex, anthropometric variables and, occupation, had been reported by Shaheen et al. [11]. A study conducted by Dhananjaya et al. [12] reported a negative correlation between handgrip strength and BMI. Shaheen et al. [11] established the normative values of handgrip strength and pinch strength using the Jamar dynamometer and pinch meter as they showed accurate measurements. The MyoGrip was compared with the Jamar dynamometer to prove its reliability and establish normative values of handgrip strength [8]. Also, the MicroFET3 dynamometer was compared with the Jamar dynamometer to prove its validity in measuring the handgrip strength [13]. Still, certain limitations and disadvantages of the equipment remained, such as that they do not include the data logging features for permanent storage of the data, do not have a real-time statistical analysis feature, and that they provide measurements of handgrip strength and pinch strength without permanently storing the data for accurate documentation purposes. Also, they should be used under the supervision of a physical therapist, occupational therapist or clinical practitioner. Just like the Jamar dynamometer and the pinch meter, this device measures the hand-grip and pinch strength, but unlike the Jamar dynamometer and the pinch meter, it helps to measure the handgrip and pinch strength with the same device, as it is a dual-purpose dynamometer. The device is portable, compact and digital, can be easily handled, and is lightweight and convenient to use for all individuals. Also, the device facilitates data logging features used for statistical analysis and research purposes. The device is called a Bluetooth-enabled smart hand dynamometer because it connects to a smartphone via Bluetooth, and the data is stored in a mobile application for further analysis and research purposes. The device will also be cost-effective, so can be used in numerous hospitals and clinical setups to measure the handgrip strength and pinch strength as a fundamental hand function. Other devices available have certain limitations, such as that none are dual purpose as they measure handgrip strength and pinch strength using two different instruments. They need the supervision of an expert and do not contain data logging features or real-time statistical analysis. Also, they are not easily available except in hospitals, research centres, and medical institutes due to their high cost. With all this in mind, the Bluetooth-enabled smart hand dynamometer studied can be recommended for measuring handgrip strength and pinch strength. It can be used by the same tester as the results showed good intra-rater reliability in measuring handgrip strength and pinch strength in the dominant and nondominant hands. In the future, the inter-rater reliability of the newly designed equipment will be reported. The study will be conducted on patients to measure the HGS and PS. Normal values of HGS and PS can be found using the newly designed equipment.