Introduction
Neck pain has become a prevalent issue worldwide since 1990 [1]. In 2019, the Western and Asian countries had the highest rates of this condition per 100,000 people, based on age-standardised years lived with a disability [2]. Moreover, this condition is the second most prevalent cause, along with lower back pain, of years lived with a disability in young adults [3]. Specifically, neck pain can be caused by various biological and psychological dangers such as age, heredity, medical background with musculoskeletal condition, worry, and trauma [1, 4–6].
Non-specific neck pain is defined as a type of neck pain that is not caused by any specific underlying disease or anatomical abnormality; its symptoms can vary and may change over time [7]. In addition, a number of variables, including female sex, ageing, high job expectations, prolonged use of computers, perceived stress, inadequate social or professional support, smoking cessation, and a history of low back or neck diseases, might contribute to the appearance of non-specific neck pain [8, 9]. Non-specific neck pain can be categorised into three types: acute (lasting less than 7 days), subacute (lasting less than 3 months), and chronic (lasting 3 months or more) [10]. Previous research has shown that various forms of exercise, such as resistance training, motor control exercises, and stretching, can be effective for individuals with this condition. The research also emphasises the importance of implementing these exercises with longer duration and increased frequency to achieve optimal outcomes [11]. Due to the unknown causes of this condition, identifying accurate and reliable assessments is crucial to guide effective exercise.
Muscle fat infiltration refers to the abnormal accumulation of fat within the muscle tissue, which has been associated with poor outcomes in cervical injury, lumbar intervertebral disk degeneration, and lumbar spinal stenosis [12–14]. The potential sources of muscle fat infiltration encompass lack of use, muscle degenerative diseases, nerve irritation, and demyelinating disorders [15–17]. Nonetheless, one characteristic that might identify people with non-specific neck problems is muscle fat infiltration [18]. Therefore, a comprehensive investigation of fatty muscle infiltration under these conditions is necessary.
Various studies have investigated muscle fat infiltration using MRI in neck pain cases, including whiplash-associated disorder (WAD), cervical myelopathy, posterior longitudinal ligament, and non-specific neck pain [18–23]. A systematic review by De Pauw et al. [24] showed evidence of FI in the flexor and extensor neck muscles in WAD. Individuals with this condition tend to exhibit greater muscle fat infiltration, specifically in the deep medial cervical muscles [14, 25]. Furthermore, a recent study has shown that individuals with chronic idiopathic neck pain have significantly higher levels of muscle FI compared to those without symptoms. This finding suggests that muscle fat infiltration could be a useful radiological marker for identifying individuals affected by this condition. Another study conducted by Huang et al. [26] found a significant correlation between the Numerical Rating Scale (NRS) scores, Northwick Park Neck Pain Questionnaire (NPQ) scores, and the percentage of FI in the flexor and extensor muscles. Additionally, a study by Grondin et al. [27] also found a moderate correlation between neck disability and the percentage of FI in the multifidus muscle among individuals suffering from non-specific neck pain for more than three months. This might suggest that dysfunction in the neck muscles can lead to pain inhibition, which may, in turn, result in FI of the stabilising neck muscles. Nevertheless, it remains uncertain as there are currently no studies that have examined the changes in muscle fat infiltration over time in individuals with this condition.
Most studies examining muscle fat infiltration related to neck issues have primarily focused on individuals experiencing specific neck pain [16, 17, 20, 22, 23, 25–28]. Conversely, only a limited number of studies have explored the relationship between muscle fat infiltration and non-specific or idiopathic neck pain [27–29]. These studies have predominantly assessed neck disability, pain levels, muscle function outcomes, and cervical lordosis. Despite these findings, a significant gap remains in our understanding of how muscle fat infiltration is associated with other neck pain features, including posture and CROM, in individuals with non-specific neck pain.
This study investigated the correlation between muscle fat infiltration and various aspects of non-specific neck pain, including pain level, neck disability, CROM, and posture. We hypothesised that the accumulation of FI in cervical muscles would correlate to neck pain features in individuals experiencing non-specific neck pain. These findings could be beneficial in shaping clinical treatment approaches, such as developing targeted physiotherapies and assessments for muscles, and provide insights into the intricate nature of chronic non- specific neck pain.
Subjects and methods
Participants
The study participants were selected from August to December 2023. Participants were included if they were aged between 20 and 40 years and had experienced mechanical neck pain for more than three months. Moreover, the participants reported a pain level of 2–8 on the NRS with mild-to-severe disability (10–64% of NDI score) and worked in front of a computer. Individuals who had previous spinal surgery, whiplash injury, those who had undergone neck pain exercises in their last 3 months, had radiating pain, numbness, upper extremity weakness, a detectable pathological spinal condition, or systemic diseases were excluded from the study.
Participants were recruited using three different methods. First, the author posted an announcement about the recruitment of research participants in a social media story (Insta-gram and WhatsApp). Second, the author sent a poster to the Line group of international students at Tokyo Metropolitan University. Finally, the author announced the recruitment of research subjects directly to second- and third-year physical therapy undergraduates at Tokyo Metropolitan University.
The participants were required to provide demographic information and complete clinical measurements, such as self-reported questionnaires, CROM, and posture evaluations, before the MRI scan. All participants provided informed consent prior to inclusion in the study.
Experimental procedure
Participants provided demographic information and completed the English or Japanese versions of the NDI [30, 31].The NDI is widely used to assess neck pain conditions and exhibits excellent reliability [intraclass correlation coefficient (ICC) = 0.88; (0.63 to 0.95)] [32]. The NDI consists of ten items that assess the impact of neck pain on daily activities. These include pain, self-care, carrying objects, reading, headaches, focus, driving, sleeping, and leisure. Each item is scored on a rating scale of 0–5. The score of this questionnaire is calculated by adding the points of all items and dividing them by 50. The final score is expressed as a percentage, ranging from 0 to 4 points (0–8%) for no disability, 5–14 points (10–28%) for light disability, 15–24 points (30–48%) for moderate disability, 25–34 points (50–64%) for severe disability, and 35–50 points (70–100%) for full disability [32].
CROM
The CROM was measured using a digital goniometer (EasyAngle goniometer). The EasyAngle digital goniometer has excellent concurrent validity and reliability with an ICC of 0.97 for CROM (95% CI = 0.95–0.98) [33]. During the study, the participants were instructed to sit with their feet hip-width apart and their hands resting on their thighs while keeping their cervical spine in a neutral position. The EasyAngle goniometer was placed ventrocranial to the right ear in the sagittal plane to measure cervical flexion and extension. For bilateral rotation, the EasyAngle goniometer was positioned cranially with respect to the ear on the opposite side of movement in the transverse plane. Finally, the EasyAngle goniometer was placed ventrocranial to the ear on the opposite side of the movement in the frontal plane for bilateral lateral flexion. Each movement was repeated three times, and after every repetition, the participant was requested to return to the starting position, which was equal to zero degrees on the EasyAngle.
Neck posture measurement
Shisei-Karte (available at: https://kartie-cloud.jp/shiseikarte/) is a Japanese website that uses artificial intelligence (AI) to assess an individual’s posture based on images. This AI is a practical and academically useful tool for posture evaluation, offering measurements of various parameters such as cervical and thoracic lateral flexion angles, pelvic tilt, knee valgus angles, and centre of gravity alignment. Its academic value lies in its ability to provide accessible, non-invasive assessments, making it suitable for studies in biomechanics and rehabilitation. Shisei-Karte has shown moderate reliability, particularly for the left knee valgus angle (ICC = 0.423, p = 0.010) and strong positive correlations for trunk lateral flexion (r = 0.747 for the right, r = 0.629 for the left) and left shoulder abduction (r = 0.585, p = 0.001) compared to the VICON motion analysis system [34]. Although certain parameters, such as cervical lateral flexion, lacked statistical correlation, the tool’s comparable mean values and standard deviations to VICON suggest accurate and consistent data capture.
In this study, the measurement was performed to analyse the posture of the head, including forward and back tilts of the head and anteroposterior misalignment. This analysis is performed to detect forward head posture. This is characterised by an excessive anterior curve in the lower cervical vertebrae and an excessive posterior curve in the upper thoracic vertebrae, which is necessary to maintain balance [35]. Three steps were involved in the analysis for each subject. First, the participants were required to register by providing basic information, such as name, gender, and height. Second, the participants’ pictures were taken in a side-face standing position. After the images were captured, the analysis results were displayed for approximately 30 s.
Muscle fat infiltration
All participants underwent a standard MRI of the cervical spine. They were asked to lie on their backs and maintain a neutral cervical spine position without any rotation, lateral flexion, or exaggerated lordosis. A neck coil was used during the examination to enhance imaging accuracy. The MRI was performed using the SIGNA Premier 3.0 T (GE Healthcare Japan) (Repetition time {TR}, 8000 ms; Excitation time, 102 ms; Voxel resolution, 0.4 × 0.4 mm; Field of view, 200 × 200 mm; Thickness, 3.5 mm).
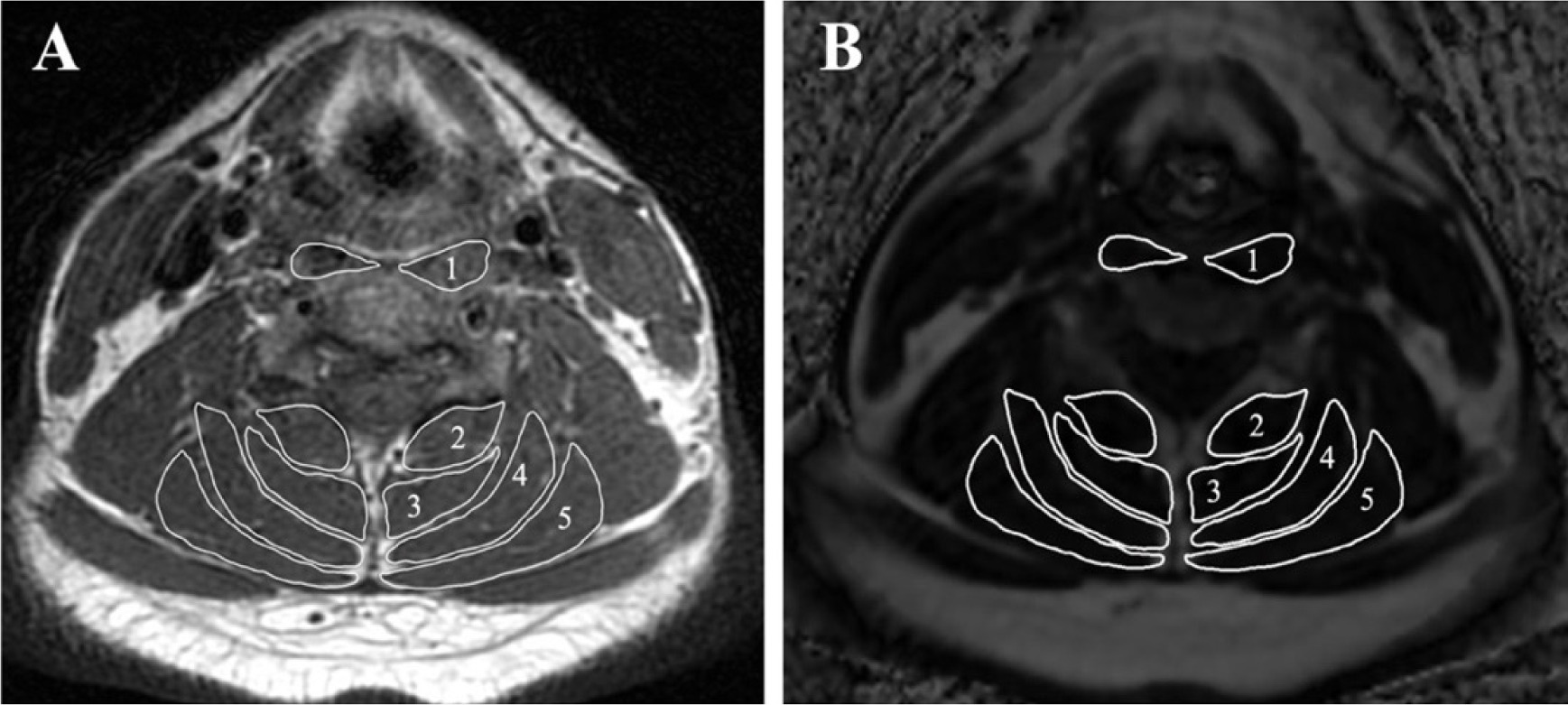
First, a T1-weighted sequence was used to enhance the fatty tissue signal and suppress the water signal. Using the Miele-lxiv image processing software (available at: https://miele-lxiv.macupdate.com/), regions within the facial borders of the longus colli and capitis (LCo & LCa), multifidus (MF), semispinalis cervicis (SSCe), semispinalis capitis (SSCa), and splenius cervicis and capitis (SpCe & SpCa) were manually drawn (Figure 1). After mapping the specific muscles in the T1-weighted sequence, the fat fraction image was used to quantify FI in each muscle. The software calculates the average signal intensity for fat accumulation in each area of interest. The mean of the bilateral muscles at C2/3, C4/5, and C6/7 was used to define the total FI.
Figure 1
Evaluation of muscle fat infiltration at C4/5. (A) T1-weighting image, (B) fat fraction image using the threshold technique with the Miele lxiv. The following measured muscles were included: 1 – longus colli and capitis, 2 – multifidus, 3 – semispinalis cervicis,4 – semispinalis capitis, and 5 – splenius cervicis and capitis
Statistical analysis
The means and standard deviations of the clinical and demographic data were calculated. The Kolmogorov-Smirnov test revealed that the measured FI data did not follow a normal distribution (p < 0.05). Spearman’s rank correlation was used to examine the correlation between muscle fat infiltration and neck pain features, including pain level, neck disability, CROM, and posture. Correlation coefficients were categorised as very high (0.90–1.00), high (0.70–0.90), moderate (0.50–0.70), or low (0.30–0.50). The critical value for statistical significance was set at p < 0.05. All statistical analyses were conducted using IBM SPSS Statistics 27.0.1.
Results
Of the 15 volunteers, 13 were selected for the study, comprising 5 men and 8 women. One participant was excluded because of neck pain with radiating pain, and another participant’s MRI data were unclear.
The demographic information and basic descriptions of the measured parameters are presented in Table 1. The mean participant age was 27.3 ± 4.4 years (range, 21–36 years). The mean NRS score for neck pain was 5.0 ± 1.7, and the mean NDI score was 17.0 ± 7.0%.
Table 1
Demographic data and clinical features (n = 13)
Bivariate correlation analysis showed a moderate correlation between the NRS score and FI in the deep extensor muscles. A significant positive correlation was observed between the multifidus’s FI at the C4/5 level (r = 0.563; p = 0.046) and the NRS score (p < 0.05; Table 3).
This study revealed correlations between the FI and CROM flexion in all measured cervical muscles. At the C2/3 level, a positive correlation was observed between FI and five muscles, including the LCo & LCa (r = 0.747; p = 0.003), MF (r = 0.601; p = 0.030), SSCe (r = 0.614; p = 0.025), SSCa (r = 0.579; p = 0.038), and SpCe & SpCa (r = 0.625; p = 0.022) (Table 2). However, at the C4/5 level, only the LCo & LCa was correlated with FI changes (r = 0.747; p = 0.003) (Table 3).Unlike C4/5, accumulation of FI was observed in the SpCe & SpCa at the C6/7 level (r = 0.554; p = 0.050) (Table 4).
Table 2
Correlation of fatty infiltration and neck pain features at C2/3
[i] NRS – numerical rating scale, NDI – neck disability index, CROM – cervical range of motion, FBTH – forward and back tilt of the head, APM – anteroposterior misalignment, LCo & LCa – longus colli and capitis, MF – multifidus, SSCe – semispinalis cervicis, SSCa – semispinalis capitis, SpCe & SpCa – splenius cervicis and capitis * statistically significant at the 0.05 level, ** statistically at the 0.01 level, ^ moderate correlation, ^^ strong correlation
Table 3
Correlation of fatty infiltration and neck pain features at C4/5
[i] NRS – numerical rating scale, NDI – neck disability index, CROM – cervical range of motion, FBTH – forward and back tilt of the head, APM – anteroposterior misalignment, LCo & LCa – longus colli and capitis, MF – multifidus, SSCe – semispinalis cervicis, SSCa – semispinalis capitis, SpCe & SpCa – splenius cervicis and capitis * statistically significant at the 0.05 level, ** statistically at the 0.01 level, ^^ strong correlation
Table 4
Correlation of fatty infiltration and neck pain features at C6/7
[i] NRS – numerical rating scale, NDI – neck disability index, CROM – cervical range of motion, FBTH – forward and back tilt of the head, APM – anteroposterior misalignment, LCo & LCa – longus colli and capitis, MF – multifidus, SSCe – semispinalis cervicis, SSCa – semispinalis capitis, SpCe & SpCa – splenius cervicis and capitis * statistically significant at the 0.05 level, ^ moderate correlation
The FI in the SSCa at the C2/3 level exhibited a positive correlation with head posture, which was moderately and positively correlated with neck posture. This significant data lies in its quantitative measurements of cervical alignment, particularly focusing on forward and back tilting of the head (r = 0.558; p = 0.048) (Table 2). The study found that the average degree of FBTH among participants was 2.4° (Table 1), indicating a slight forward displacement of the head in relation to the body’s vertical axis. In contrast to other neck pain features, only NDI scores were not significantly correlated with FI in any measured cervical muscle (p > 0.05).
Discussion
This study examined the relationship between FI and neck pain features, including pain level, neck disability, CROM, and neck posture. A decrease in range of motion, cervical mis-alignment, and neck pain can all result from dysfunctional cervical spine muscles [36, 37]. Research has shown that the accumulation of FI in muscles can have detrimental effects on various spinal conditions, such as disc herniation, disc disease, and unilateral lower back pain [26, 29, 38–40].
We found that the FI in the multifidus muscle at the C4/5 level exhibits a moderate and significant correlation with pain level measured by the NRS score. In particular, a correlation was found between more severe neck pain and more FI existing in the mid-cervical extensors. This is supported by the studies by Kim et al. [41] and Snodgrass et al. [18], which revealed that FI in the cervical extensor muscle was associated with high visual analogue scale scores. Moreover, the research conducted by Huang et al. [26] found a correlation between NRS score and fat accumulation within the right extensor muscles. The multifidus muscle is part of the neck extensor group and is located anteriorly among cervical paraspinal muscles [42]. Muscle dysfunction at a deep level can result in weakened muscles and the accumulation of fat around them, which can result in heightened discomfort. However, as this study was cross-sectional, it could not determine whether the fat grade causes the pain or is a result of this pain. Furthermore, studies have suggested that healthy individuals experience an increase in FI after four weeks of immobilisation [31], while older people can exhibit decreased FI accumulation in thigh muscles after 12 weeks of strength exercise [43]. Based on these findings, future studies should explore interventions that may reduce FI in the deep extensor cervical muscles to assess their effects on neck pain.
To the best of our knowledge, this is the first study to investigate the correlation between FI and CROM in patients with non-specific neck pain. Previous studies have examined fat accumulation and range of motion in the shoulder and lumbar spine [44, 45]. According to a study conducted by Hildebrandt et al. [45], the range of motion in the lumbar flexion decreased significantly as the severity of FI in the lumbar multifidus muscles increased. Conversely, this study discovered that an increase in FI in neck muscles may lead to enhanced CROM flexibility, particularly in flexion. Cooper and Daniel [46] explained that the deep muscles of the upper spine play a vital role in stabilising the head and neck. Therefore, we suggest that the accumulation of FI in the flexor and extensor muscles may cause instability. However, our study did not investigate joint instability; further research is required to examine this aspect.
This recent result seems to contradict the findings of Hildebrandt et al. [45], which could be attributed to differing methodologies. While they measured both acute and chronic stages, this study focused solely on the chronic stage [45].
According to this study, there is a significant positive correlation between FI in the SSCa muscle at C2/3 and neck posture, specifically in the forward and back tilts of the head. This indicates that a greater amount of FI into the cervical area can affect the position of the head. This finding was supported by Lee et al. [47], who found that patients with a degenerative lumbar flat back exhibited significantly greater FI compared to the normal control group. Moreover, Harrison et al. [48] explained that cervical lordosis can be lost due to diminished size and strength of the cervical extensor muscles from increased FI. This condition may worsen with axial stress on the cervical spine, causing high tension in the posterior neck muscles as well as around the upper part of the back, leading to neck discomfort. Similarly, an axial load moving forward can persistently strain the posterior neck musculature, fatigue the cervical extensors, and cause flattening of the cervical spine. The interplay among these factors can lead to a vicious cycle of pain and muscle weakness [48, 49]. Furthermore, Panjabi [50] explained the description of a three-subsystem model of spinal stability: the neural motor unit, vertebral muscles, and vertebral column. Together, these subsystems produce the ideal balance between dynamic stability and spinal flexibility. Because of their interdependence, if one system is compromised, the other can make up for its shortcomings. However, if neck pain occurs, neural control is inhibited, affecting the activity of the alpha motor neurons in the anterior horn of the spinal cord and neck muscles.
Apart from CROM-related movement and posture, another key factor associated with cervical pain is muscular condition, encompassing muscle strength, endurance, and size [51, 52]. Research indicates that individuals with mechanical neck pain often demonstrate significant weakness in their neck flexor muscles, which contributes to their pain and discomfort [53, 54]. However, there is currently no evidence linking neck muscle strength or mobility to the development of neck pain or disability later in life [55]. Furthermore, while muscle endurance is correlated with neck pain, a previous study found no association between neck disability in individuals with idiopathic neck pain and muscle fat infiltration in the neck flexors [27]. It is worth noting that this study examined a limited number of neck muscles, indicating that further investigation in this area would be both reasonable and necessary.
Compared with other neck pain features, only the neck disability parameter was not found to have any significant correlation with the FI at any cervical level or specific cervical muscles. Previous studies have shown a moderate and significant correlation between NDI and NPQ scores and the percentage of FI in the multifidus in people with non-specific neck pain and idiopathic neck pain [26, 27]. It is possible that the current study produced different results because the participants had mild disability levels; there appears to be no significant correlation between this particular factor and the presence of FI. Moreover, a smaller sample size might indicate that the results had less precision and lower statistical power compared to the previous study [27], which benefited from a larger sample size. Further investigation is essential to enhance our understanding of this matter.
Limitations
This study has some limitations that must be acknowledged. Since it was a cross-sectional study, causality was not established – only correlations. Additionally, there might be a potential for bias in this single-centre study, as there was only one tester and one reviewer. Furthermore, visual analysis was employed to assess the accumulation of FI in the cervical muscles, acknowledging the limitations of this method. Additionally, the authors recognise potential inaccuracies in the MRI methodology, especially in the muscle mapping. Moreover, potential differences may exist between males and females – such as variations in muscle fat infiltration, pain level, disability, CROM, or posture. These were not captured or analysed due to limitations in the study’s design and sample size. Future research involving larger and more balanced participant groups may provide a more comprehensive understanding of these differences.
Furthermore, the validity of the Shisei-Karte posture assessment tool has not yet been established in peer-reviewed academic studies. The available reference is based on a conference abstract, which limits the certainty of its reliability. Future research should focus on validating this tool through rigorous studies before widespread adoption in clinical and research settings.
Conclusions
This cross-sectional study based on MRI established correlations between muscle fat infiltration and neck pain features such as pain, neck disability, CROM, and posture. There were strong and moderate correlations of the pain level, CROM, and forward head posture with fat accumulation in the cervical muscles. Conversely, no significant relationship was found between neck disability and muscle fat infiltration at the cervical level. This study suggests a potential for developing muscle-specific physiotherapies and assessments to improve treatment strategies for chronic non-specific neck pain.