Dear Editor,
I read with great interest the study by Ismail et al. [1] on the effectiveness of capacitive and resistive electric transfer (CRET) in non-specific chronic low back pain. The investigation of radiofrequency-based electromagnetic modalities is particularly relevant given their growing application in musculoskeletal rehabilitation [2, 3]. Notably, the inclusion of a wide range of recognised electronic databases in this systematic review (SR) reflects best practices in evidence-based research [4]. Although CRET therapy is widely used across the globe, a comprehensive understanding of its efficacy and underlying mechanisms still requires further investigation [5].
After reviewing the article and the included studies, the available quantitative data supports conducting a meta-analysis to evaluate the effectiveness of CRET on two key outcomes [6]: pain intensity and disability. Six studies assessed pain using the Visual Analogue Scale (VAS) or Numerical Pain Rating Scale (NPRS), while four evaluated disability using the Oswestry Disability Index (ODI) and the Roland-Morris Disability Questionnaire (RMDQ) (Table 1).
Table 1
Characteristics of studies included in the CRET systematic review by Ismaili et al. [1]
| Nº | Author (year) [reference in the SR] | Indexed in PEDro database | Participants (n) mean age (SD) | Groups (n) | Sessions | Outcomes | Assessment instance | Conclusion | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Tashiro et al. (2020) [13] | no | 30 (M = 8, F = 22) 33.3 (NS) years dropout 1 not received allocated intervention 3 | EG (11): CRET + EX CG (15): EX | 2–3 s/ week for 4 weeks | (A) pain intensity (VAS)* (B) disability (ODI)** (C) flexibility (KWT) | T0: baseline T1: post-treatment (4 weeks) T2: follow-up (4 weeks) | Exercise alone was less effective in treating NSCLBP than CRET plus exercise. | ||
| 2 | Wachi et al. (2022) [23] | no | 24 (M = 24, F = 0) 33.4 (8.1) years dropout 0 | EG (12): CRET CG (12): sham CRET | 1 s | (A) pain intensity (VAS)* (B) muscle stiffness (USG) (C) muscle activity (EMG) | T0: baseline T1: post-treatment | CRET provided acute benefits for NSCLBP and muscle stiffness. Further research is needed on its effects on spinal tissues and its combination with exercise. | ||
| 3 | Wachi et al. (2022) [22] | no | 30 (M = NS, F = NS) 33.4 (9.8) years dropout 0 | EG (15): CRET CG (15): sham CRET | 1 s | (A) pain intensity (VAS)* (B) muscle activity (EMG) | T0: baseline T1: post-treatment | CRET therapy reduced pain and enhanced trunk muscle activity, potentially improving daily functioning. | ||
| 4 | Lee et al. (2022) [26] | no | 118 (M = 26, F = 92) 47.7 (7.3) years dropout 14 | EG (56): CRET CG (48): US | 3 s/ week for 4 weeks | (A) pain intensity (NPRS)* (B) trunk extensor strength (BST) (C) disability (ODI)** (D) function (TUG) (E) satisfaction (NASS) | T0: baseline T1: post-treatment (4 weeks) T2: follow-up (12 weeks) | CRET improved pain, function, mobility, and endurance, with similar effects to US but slightly better pain relief at 12 weeks. It may be a conservative treatment for LBP. | ||
| 5 | Kasimis et al. (2023) [27] | yes | 60 (M = 20, F = 40) 38.4 (2.5) years dropout 1 | EG (20): CRET plus MT CG1 (20): MT CG2 (20): no treatment | 3 s/ week for 2 weeks | (A) pain intensity (NPRS)* (B) PPT (ALG) (C) disability (RMDQ)** (D) function (FTFT) | T0: baseline T1: post-treatment (2 weeks) T2: follow-up (4 weeks) | MT plus CRET improves pain, disability, local sensitivity, and lumbo-pelvic mobility in CNSLBP, likely due to combined mechanical and thermal effects. | ||
| 6 | Zati et al. (2018) [24] | yes | 49 (M = 23, F = 26) 60.0 (11.2) years | EG (25): CRET CG (24): SHT | 5 s/ week for 2 weeks | (A) pain intensity (NPRS)* (B) disability (ODI)** | T0: baseline T1: post-treatment (2 weeks) T2: follow-up (4 weeks) T3: follow-up (6 weeks) | CRET is effective for NSCLBP and may aid in multidisciplinary management. | ||
| 7 | Barassi et al. (2022) [25] | no | 40 (M = NS, F = NS) 23.2 (2.5) years | EG1 (20): CRET (resistive mode preceded capacitive) EG2 (20): CRET (capacitive mode preceded resistive) | 1 s | (A) PPT (ALG) (B) tissue temperature (thermal imaging) | T0: baseline T1: post-treatment | CRET reduces LBP, with minimal benefit from starting with resistive mode. |
[i] ALG – algometry, BST – Biering-Sørensen test, CG – control group, CRET – capacitive and resistive electric transfer, EMG – electromyography, EG – experimental group, EX – exercise, F – females, FTFT – Fingertip-to-Floor test, KWT – Krauss Weber test, LBP – low back pain, M – males, NASS – North America Spine Society 4-point patient satisfaction index, NPRS – Numeric pain rating scale, NS – not specified, NSCLBP – non-specific chronic low back pain, ODI – Oswestry Disability Index, RMDQ – Roland-Morris Disability Questionnaire, SHT – Superficial Heating Therapy, SR – systematic review, TUG – Timed up-and-go test, US – therapeutic ultrasound, USG – ultrasonography, VAS – Visual analogue scale * outcome included in the pain intensity meta-analysis ** outcome included in the disability meta-analysis
Therefore, this letter aims to further examine the effectiveness of CRET in reducing pain and disability by performing a secondary meta-analysis of the studies included in the SR by Ismail et al. [1]. Pain changes were evaluated by statistically pooling the results of the VAS and NPRS, while disability changes were assessed by grouping the ODI and RMDQ, using standardised mean differences (SMDs) due to the differing nature of the instruments [7, 8]. The overall effect was estimated using Cohen’s d effect size. Depending on the observed heterogeneity (I2 50%), either a fixed-effects model (Mantel-Haenszel) or a random-effects model (DerSimonianLaird) was applied (Figure 1) [6, 9].
Figure 1
(1A) Forest plot for pain intensity at the end of treatment: Comparison of CRET versus control (exercise, sham CRET, therapeutic ultrasound, manual therapy, or superficial heating therapy) after treatment (Fig. 1.1.1); CRET versus control (exercise, therapeutic ultrasound, or superficial heating therapy) for the follow-up period (Fig. 1.1.2). (1B) Forest plot for disability at the end of treatment: Comparison of CRET versus control (exercise, therapeutic ultrasound, manual therapy, or superficial heating therapy after treatment) (Fig. 2.1.1); CRET versus control (exercise, therapeutic ultrasound, or superficial heating therapy) for the follow-up period (Fig. 2.1.2)
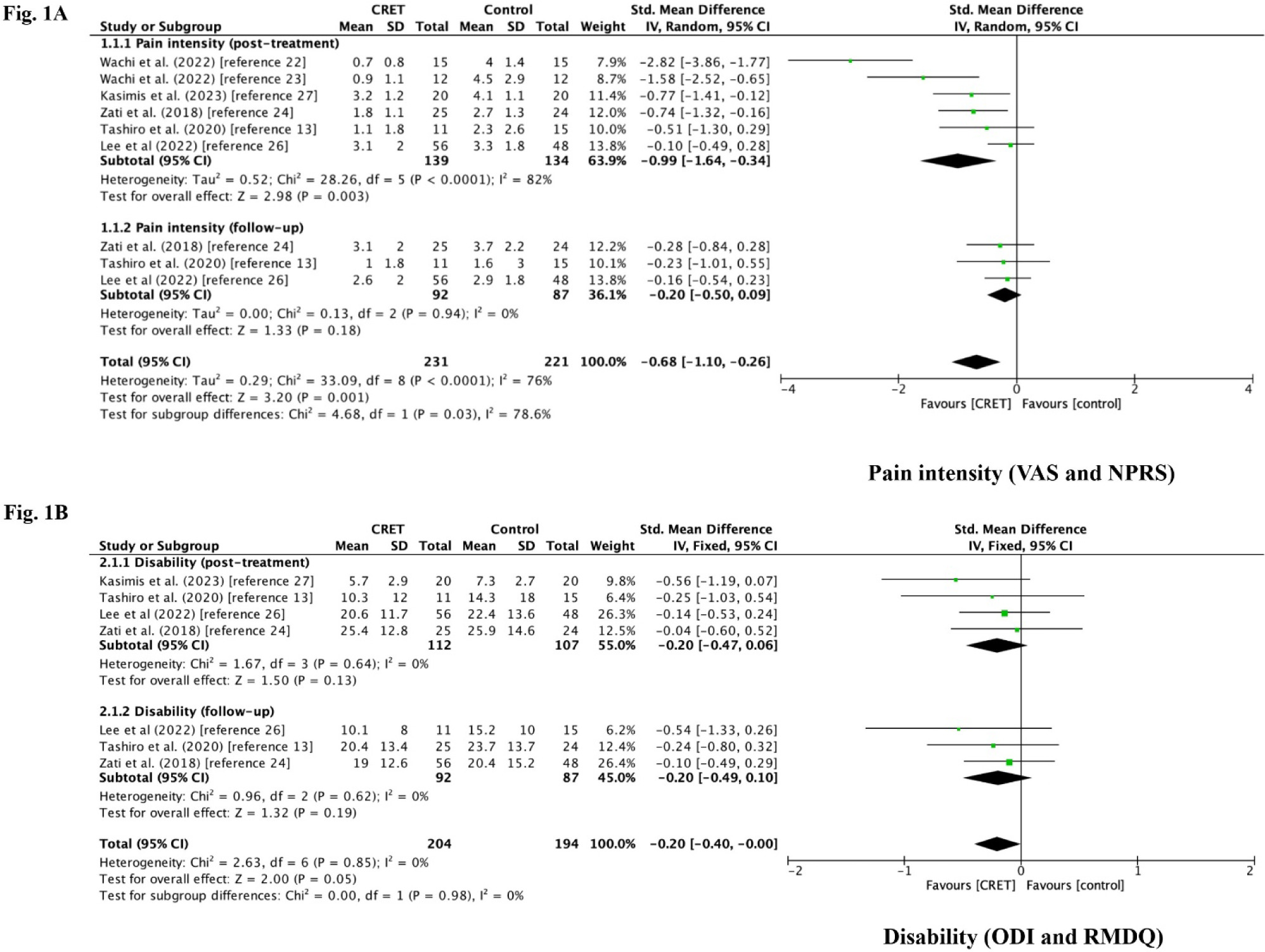
The results indicate that CRET demonstrates superiority over control interventions in terms of short-term pain reduction (exercise, therapeutic ultrasound, manual therapy, or sham CRET) at the end of treatment, with a large effect size [SMD = –0.99; 95% CI: –3.4, –1.6; p < 0.01; CRET (n = 139), control (n = 134)]. However, during follow-up periods ranging from 4 to 12 weeks, the effect size was small (d = –0.2) and not statistically significant (Figure 1A). Regarding disability, no statistically significant differences were observed either at the end of treatment or during follow-up, with a similarly small effect size (d = –0.2) (Figure 1B). Therefore, these findings suggest that CRET is effective only for short-term pain reduction, without a significant impact on disability, which refines the authors’ conclusions regarding its effectiveness in chronic low back pain.
Furthermore, several methodological concerns should be addressed. The authors claim to have followed PRISMA guidelines; however, they do not provide protocol registration or indicate its availability (items 24a–24c of the PRISMA checklist) [10, 11].
The design of the study is not clearly specified, despite reference to the PICOS framework. Although the review appears to include only randomised controlled trials on CRET, one study without a control group (Barassi et al.) was included, where both groups received CRET (Table 1). According to the authors’ PICOS criteria, this study should be excluded due to the lack of a valid comparison between CRET and other treatments.
There is a discrepancy in the PEDro score of the Barassi et al. study. The PEDro database lists it as 8, while the authors report it as 7 due to assessor blinding, which is documented in the original article.
The review does not specify the date of the last search update. While the study was accepted on April 6, 2024, and this could be inferred as the last update date, Cochrane guidelines recommend updating the search within a year of publication, so an update is advised [6, 12].
The authors used the Cochrane Risk of Bias tool but did not include the ‘traffic light plot’ to visualise individual study quality assessments alongside the ‘summary plot’ [6, 13].
The concurrent use of the PEDro scale to assess methodological quality and the Cochrane Risk of Bias tool to evaluate risk of bias introduces methodological redundancy, as both instruments address overlapping domains of internal validity. In SRs, it is standard practice to apply a single validated tool for the assessment of study quality or risk of bias. Additionally, the methodology does not report the use of the PEDro scale, despite it being referenced in the Results section [14, 15].
Finally, the authors claim that CRET improves quality of life. However, this assertion is questionable since no studies included instruments to assess this outcome. Instead, the analysis focused on disability and function, which are distinct from quality of life.
Despite the methodological concerns identified, the authors should be commended for addressing a therapeutic modality that is gaining increasing attention in physical therapy practice [2–4]. The decision to conduct a systematic review is particularly noteworthy, as it represents one of the most rigorous and reliable approaches to evidence synthesis. Moreover, the authors’ comprehensive assessment of the methodological quality of the included studies adds meaningful value to the current literature.
This letter seeks to complement their work by providing an additional quantitative analysis of treatment effectiveness and by offering methodological considerations aimed at strengthening the interpretation of the findings and informing the design of future high-quality clinical trials in this field.