Introduction
Musculoskeletal health encompasses the efficient functioning of the body’s movement system, and its impairment can result in temporary or permanent limitations in daily activities and social participation. These impairments manifest as chronic pain, reduced mobility, and decreased dexterity, hindering individuals’ ability to work and fully engage in community life [1].
Consequently, these conditions pose the greatest global burden on rehabilitation services. According to a 2019 analysis, over 1.71 billion individuals worldwide suffer from musculoskeletal disorders that significantly contribute to global disability, as measured by years lived with disability (YLDs) [1, 2].
The ICD-11 classifies chronic primary musculoskeletal pain (CPMP) as persistent discomfort in the muscles, bones, joints, or tendons accompanied by significant emotional distress, including anxiety, anger, frustration, or depression, and limitations in daily activities. Societally, chronic musculoskeletal pain imposes substantial financial burdens on healthcare systems, disability programs, and the economy due to increased absenteeism from work [3].
Exercise is a cornerstone of chronic musculoskeletal disorder rehabilitation, offering significant therapeutic benefits. Exercise interventions can take the form of in-session exercises, performed under supervision during the physiotherapy session in a clinical setting, or prescribed as at-home exercises. A home exercise program (HEP) is a personalised set of exercises prescribed and taught by a physiotherapist to address specific patient needs [4].
The HEP plays a vital role in recovery from various musculoskeletal disorders. Properly designed HEP targets the primary cause and facilitates recovery. Research consistently demonstrates that patient adherence to prescribed home exercise programs is often suboptimal [5, 6]. Studies on musculoskeletal conditions have revealed that non-adherence to home exercise programmes ranges from 50 to 70% [7, 8].
Understanding the factors affecting the adherence to HEPs may be useful in designing such programmes. Analysing the published research might serve as a base for further research. This scoping review encapsulates the identified factors that affect patient adherence to the prescribed exercise programs.
Subjects and methods
This scoping review adopted the frameworks proposed by Arksey and O’Malley [9] and the methodological advancement by Levac et al. [10].
The steps in this scoping review were: (1) identifying the research question, (2) literature search to scope out relevant studies, (3) screening and data extraction, (4) synthesis and tabulation of the data and, (5) report preparation.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [11] were diligently adhered to. The study did not require ethical clearance as a scoping review collates data from published studies.
The process followed the screening, inclusion / exclusion of studies with justification as depicted in the PRISMA flow chart. The extracted data was analysed and descriptively presented, with tabulations wherever feasible.
The research problem, search strategy, screening criteria and data extraction template were determined by the authors. The studies that included terms such as: (1) chronic musculoskeletal pain, (2) exercise prescription, (3) home exercises, and (4) adherence, were combined within and across search fields with the boolean operators ‘OR’ and ‘AND’, respectively. Using this strategy, the initial search was conducted in Medline (PubMed) and later adapted to the other databases.
Review question
This review investigated the scope of research on HEP adherence in patients with musculoskeletal pain. The principal query for this scoping review was:
(a) What are the factors influencing HEP adherence among patients with musculoskeletal complaints?
The scoping review also sought answers to the following secondary questions:
(b) What were the mode of delivery and monitoring for adherence?
(c) How are the identified factors grouped and applied in practice?
The eligibility criteria for research article selection were determined with the population, concept, and context (PCC) framework as below.
Population
Inclusion – patients with chronic musculoskeletal pain prescribed home exercises, assessed for adherence during or post the intervention period, with or without a note on recovery.
Exclusion – patients with chronic musculoskeletal pain advised to have or having undergone surgical management, or reporting a traumatic onset and not prescribed a home-based exercise regimen.
Concept
Studies used exercise as an intervention to manage and rehabilitate patients with musculoskeletal complaints, and observations of exercise adherence provided with descriptive reasoning.
Context
Studies conducted in any geographic location, with the context of exercise as an intervention for chronic pain.
Types of sources
Studies that were peer-reviewed and published in the English language since 2000, conducted on human subjects with qualitative and mixed-method study designs, or those studies that were conducted secondary to / within an experimental study were included as relevant. This review also considered systematic reviews and ensured data duplication was prevented due to repetition. This review did not look into grey literature.
We searched PubMed, Google Scholar, and Ovid Emcare. The preliminary search was conducted through PubMed using MeSH terms (Figure 1). Further searches in the other databases were carried out using the PubMed search criteria. The search identified 24 research papers. The identified citations were imported into the Covidence software for further screening and data extraction. Covidence automatically identified three duplicates for exclusion.
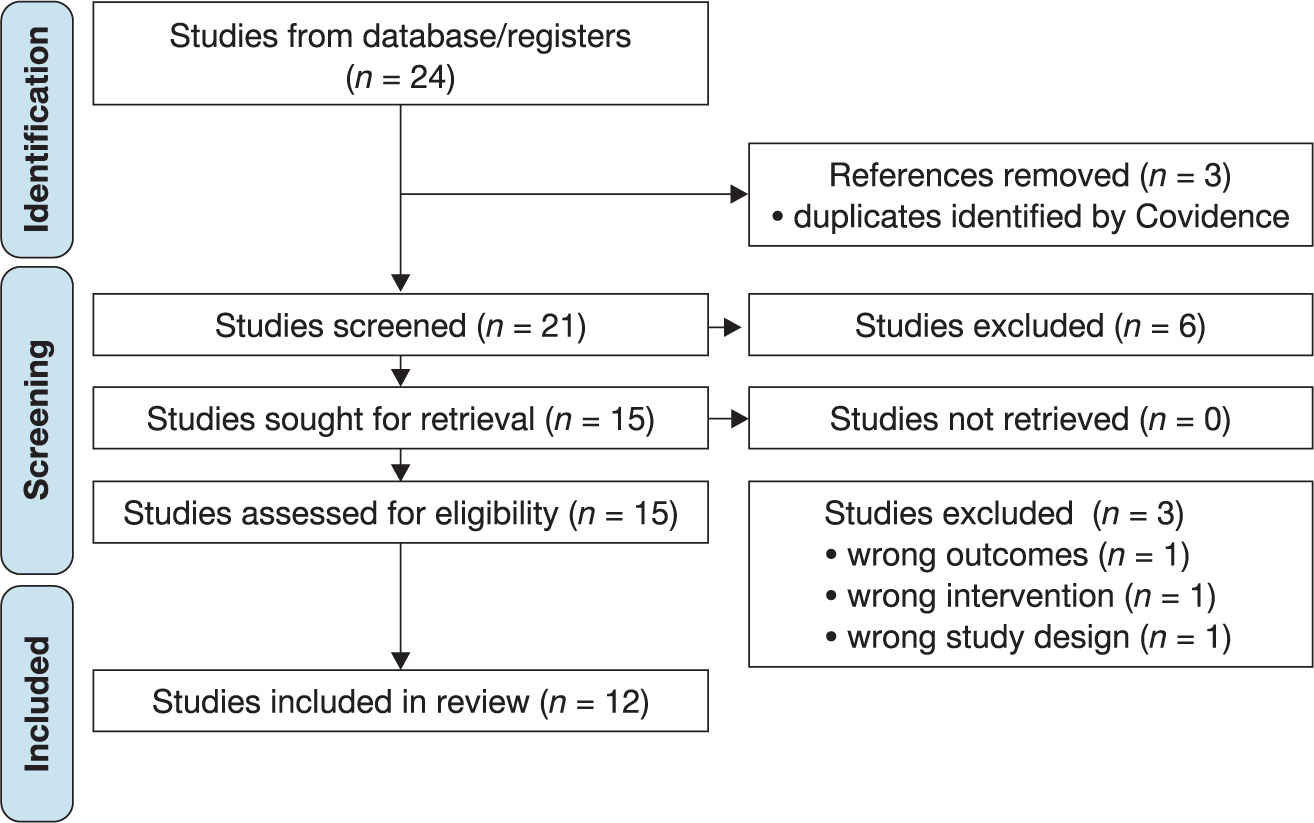
The authors independently screened the titles and abstracts. In the case of differences, the authors arrived at a mutual agreement through discussion. The screening of the 21 studies’ titles and abstracts identified 15 studies for full-text screening after the exclusion of 6 studies. The authors then independently screened the full texts. Three studies were excluded, and the reasons documented. The reasons for exclusion of the full text papers were: (1) wrong study design (the study looked into the efficacy of various health interventions for adherence rather than the factors for adherence), (2) wrong intervention (the study utilised counselling as an intervention to look into its effect on adherence) and, (3) wrong outcomes (the study looked at the rate of patients’ return to care instead of the rate of adherence). This resulted in the inclusion of 12 studies for data extraction.
Data extraction
We used a pre-determined template to extract data from the 12 included studies. Author SJV carried out the data extraction, and NS crosschecked for accuracy. The discrepancies were resolved through consensus reached by discussion. The data extracted includes specific details about the lead author, year and geographic location of the study, methods and participants, outcomes and the adherence factors identified. The extracted data was analysed in Microsoft Excel, and the aggregated data represented in graphical or tabulated formats to suit the review’s objectives.
Results
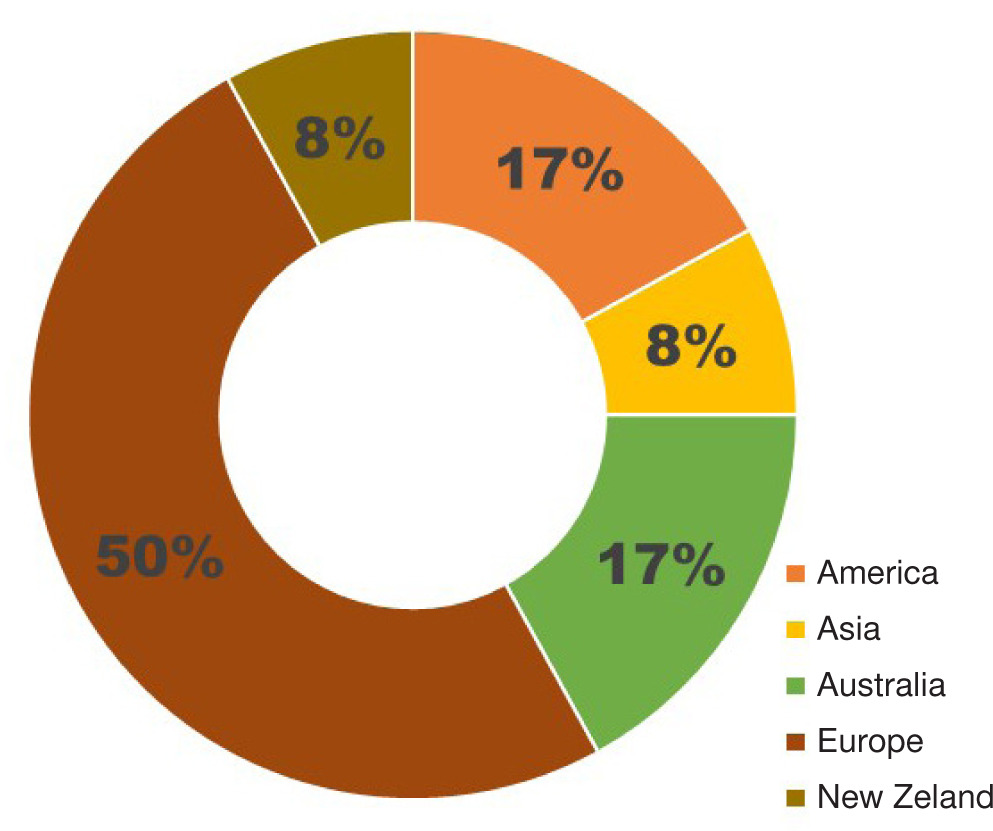
Out of the 21 studies identified, 12 studies were included for data extraction after title, abstract and full-text screening, based on the eligibility criteria. Most of the included studies are from Europe, with four studies conducted in the United Kingdom, two in other European countries, and two in Australia. The Americas reported two studies, while Asia and New Zealand reported one study each (Figure 2).
The included studies presented the variability of patient adherence to the prescribed home exercise regimen and its multifactorial nature (Table 1). Two of the 12 studies presented suggestions to improve patient adherence to the exercise programs.
Table 1
Demography, study type and identified determinants of adherence
| Lead author, year, country of origin | Type of study | Determinants of adherence |
|---|---|---|
| Kumarasamy et al., 2019 [4] Malaysia | qualitative study | multifactorial, classified as enablers and barriers |
| Beinart et al., 2013 [5] UK | systematic review | – health locus of control – supervision – participation in an exercise program – participation in a general behaviour -change program incorporating motivational strategies |
| Bassett et al., 2003 [7] New Zealand | text and opinion | variables of patient personal characteristics, disease /injury, treatment, and patient-practitioner relationship |
| Medina-Mirapeix et al., 2009 [12] Spain | qualitative study | – beliefs about illness and adherence – perceptions in relation to barriers, social and physical environment |
| Jack et al., 2010 [13] UK | systematic review | – levels of physical activity at baseline – self-efficacy – social support – pain levels during exercise |
| Moore et al., 2020 [14] UK | qualitative study | – participants’ perceptions of the interventions – knowledge about the role of exercise in pain – perceived progress / benefits – therapeutic alliance between patient and practitioner |
| Nava-Bringas et al., 2016 [15] Mexico | prospective, observational study | lack of time, pain, and fatigue |
| Campbell et al., 2001 [16] UK | qualitative study | varies at initial stage, and continued adherence at the later stage |
| Wright et al., 2014 [17] Australia | cross-sectional study | patient-practitioner relationship |
| Peek et al., 2016 [18] Australia | systematic review | – activity monitor and feedback system – written exercise instructions – behavioural exercise programme with booster sessions – goal setting |
| Palazzo et al., 2016 [19] France | qualitative study | – exercise program – healthcare journey – patients’ representations – the environment |
| Azevedo et al., 2021 [20] Brazil | secondary analysis of RCT | patient independence in performing the exercises |
A comprehensive analysis of the factors influencing patient adherence revealed three primary categories (Table 2):
Patient-centric factors / pati ent characteristics
Intervention-centric factors / intervention characteristics
Practitioner-centric factors / practitioner characteristics
The included studies described how each identified category of factors influenced exercise adherence, and their interconnected nature. These factors are summarised in Table 2.
Table 2
Factors affecting adherence to home exercises
Overall, the identified factors in each of the three categories could be characterised as either an ‘Enabler’ – promoting adherence, or a ‘Barrier’ – hindering adherence [4]. The most commonly observed enablers included the patients’ self-motivation and a positive view of exercises, a tailor-made exercise regimen, and collective adherence within groups. The barriers observed were the level of pain, and the patient’s lack of time, motivation, and self-efficacy. This review also identified that a majority of these factors act as both enablers and barriers, depending on the biopsychosocial nature of the patient and the interventional approach by the practitioner. The observed dual nature of the influencing factors was such that factors that were enabling at the onset of the intervention turned into barriers with time with the changing perceptions and expectations of the patients and vice versa.
Discussion
Suboptimal adherence to a prescribed HEP is universal, irrespective of the age, gender, and pain characteristics of the patient population [21]. Adherence can be elucidated by the dynamic biopsychosocial nature of the patient and the interventional approach of the practitioner.
Twelve studies investigated the factors affecting optimal patient adherence to the prescribed HEP. Two of those studies also investigated and put forth suggestions and aids to sustain and/or improve the level of adherence.
Medina-Mirapeix et al. [12], Jack et al. [13], and Moore et al. [14] found a significant association with the levels of pain and patient awareness on the role of exercises in pain relief.
The analysis observed that the presence and duration of pain, and/or its reduction or absence for an extended period, altered the patients’ tendency to exercise. Nava-Bringas et al. [16] also reported on the role of patient pain and fatigue towards exercise performance.
The patient-practitioner relationship is one of the key predictors of exercise adherence, as reported by Bassett et al. [7], Campbell et al. [16], Moore et al. [14] and Wright et al. [17]. The relationship is predictably influenced by patients’ assessments of the practitioner’s productivity, communication, and trustworthiness during consultations.
Campbell et al. [16] also put forth the ‘Model of Continued Compliance’, according to which the initial adherence is a result of a positive view of physiotherapy, obligation towards the practitioner and dislike of prescription medicines. In contrast, continued, long-term adherence is due to the interplay of the patients’ symptoms, perceived effectiveness, motivation, and the ease of incorporating the prescribed exercises into their lifestyle. The greater the congruence between an exercise regimen and a patient’s lifestyle, the higher the likelihood of adherence [21].
Peek et al. [18] and Palazzo et al. [19] reported that implementing an active monitoring and feedback system with periodic patient follow-up that eased contacting the practitioner improved adherence. While the former noted that providing written instructions [22] for exercises with adjunct behavioural sessions to inculcate goal setting and motivation yielded better adherence, the latter reported that making the exercise regimen more attractive while evoking a feeling of social support aided in improving adherence. Beinart et al. [5] similarly concluded that supervision by the practitioner, and patient participation in a behavioural change program that incorporates motivational strategies positively promote adherence. Regular follow-up with feedback, and motivational sessions are an effective aid for continued adherence. This can be implemented with the use of technological aids for follow-up and motivation through virtual coaching [23].
Exercise adherence can also be attributed to the patients’ perceived independence in performing the exercises, rather than strictly following the exercise guidelines [12] as it may evoke a sense of self-motivation and self-efficacy. A person-alised exercise prescription, with a detailed explanation of the exercises, improves the patients’ perceptions of exercise as an intervention and the tendency to adhere to them [22].
Adherence to the prescribed HEP might influence the outcome positively. The studies showed that the outcomes were better in clients who adhered to the HEP compared to the non-adherence population [24, 25]. The consequences of a lack of adherence include increased cost and reduced treatment effectiveness. It might also increase the burden on the healthcare system [13]. Thus, it is essential to understand the factors influencing patient adherence to devise strategies to improve compliance and overall treatment outcomes.
The scoping review has identified the multifactorial nature of patient adherence to a prescribed HEP, and the possible improvement strategies. Further research in the field can seek to investigate a more diverse population across the globe, and the feasibility and efficacy of the suggested strategies.
Limitations
Only three electronic databases were utilised to identify research papers, and grey literature was excluded, which could have resulted in limited number of studies. Furthermore, studies investigating the adherence to physical activity could not be included owing to their study of the healthy population, as this study aimed to identify the influential factors among patients with chronic musculoskeletal pain. This review was limited to publications in the English language, potentially excluding relevant research conducted in other languages.