Introduction
CoVid-19 was declared a pandemic in March 2020 by the World Health organization (WHo), and the entire world implemented various measures to reduce the spread of the disease [1]. The impact of this virus has been catastrophic, with over 6 million deaths worldwide [2]. A previous literature review concluded that healthcare workers suffered psychological and health complications when dealing with CoVid-19 [3]. despite realising that in May 2022, most countries have transitioned from a pandemic to an endemic state, the level of vigilance regarding the spread of CoVid-19 remains high, while continuing to apply health protocols in daily life [4].
Previous studies showed that CoVid-19 can cause multi-organ damage, resulting in a wide spectrum of clinical manifestations [5–7]. Furthermore, cardiovascular (CV) complications are significant concerns in the pathophysiology of the disease and are often observed as the main cause of death [7]. Experts concluded that the presence of comorbidities increases the risk of complications due to CoVid-19 [8]. Several symptoms, such as myocardial damage, myocarditis, acute coronary syndromes, respiratory syndrome, arrhythmias, and thromboembolic diseases, have been observed among individuals affected by the virus [9].
The implementation of several government policies aimed at reducing the spread of CoVid-19, such as ‘work from home’ or restrictions on physical activity (PA) [10], caused a decrease in cardiorespiratory fitness (CRF) [11]. Previous literature showed the relationship between CRF and information about health status alongside prognosis during the pandemic [12]. A 3-week cardiac telerehabilitation exercise program improved the CRF and assisted in the rehabilitation of patients with acute CoVid-19 due to a history of poor CRF [13]. To support this finding, experts concluded that CRF plays a crucial role as an indicator of the risk of CoVid-19 infection, as its insufficient levels can cause poor host immunity [14, 15].
Previous studies have reported an important correlation of CRF with the risk of being infected with CoVid-19 [16–18]. For example, Fikenzer et al. [16] conducted observations between handball athletes with and without a history of CoVid-19. The results showed that the maximal oxygen consumption (Vo2max) in healthy athletes was greater. While these discoveries may still be subject to debate, this study highlights the importance of conducting screening following SARS-CoV-2 infection to identify any performance limitations and ensure readiness for competition.
According to Fikenzer et al. [16], an improvement in CRF level, strengthens host immunity and can reduce the risk of contracting CoVid-19 in athletes. Therefore, it could also decrease the symptomatic risk of infected patients. This is supported by the notion that a robust immune response can help prevent excessive symptomatic occurrence [19]. However, there was limited literature available in this specific context. only the study conducted by Gervasi et al. [19], which focused on soccer players, compared CoVid-19 patients with asymptomatic or mild symptoms. However, it was limited to cardiopulmonary testing, and the results showed that players with mild symptoms experienced a statistically significant reduction in almost all spirometry parameters.
There has been no study comparing CRF levels in adults with asymptomatic and mild symptoms of CoVid-19. This comparison is essential as the results can help identify performance limitations and guide the safe resumption of exercise. Therefore, this study aimed to measure and compare CRF levels between adult patients with asymptomatic and mild symptoms of CoVid-19. Furthermore, it is hoped that the results can contribute to the existing scientific literature and provide relevant information to the public regarding exercise intensity recommendations during the pandemic.
Subjects and methods
Participants
The participants in this observational study were 50 adult men who were further divided equally into 2 categories: mild symptoms (MS) and asymptomatic (AS) groups. They were selected based on the inclusion and exclusion criteria. The inclusion criteria included (1) men with an age range of 40 to 50, (2) absence of musculoskeletal injuries within the last 6 months, (3) non-athletes or individuals without a history of a systematic exercise training system, (4) CoVid-19 patients who had recovered at least 3 months before the start of this study, (5) for the MS group, individuals who experienced mild symptoms such as rhinitis, breathing problems, headaches, no sense of taste and/or smell, chest pain, sore throat, cough, sniffles, listlessness, and aching limbs, and (6) for the AS group, those that did not experience any symptoms while suffering from CoVid-19. The exclusion criteria included consumption of alcohol, caffeine, supplements, and exercise in the three months preceding the study or during the experimental period. The participants were fully informed about the objectives, benefits, and risks, and they provided their informed consent before participation.
Experimental design
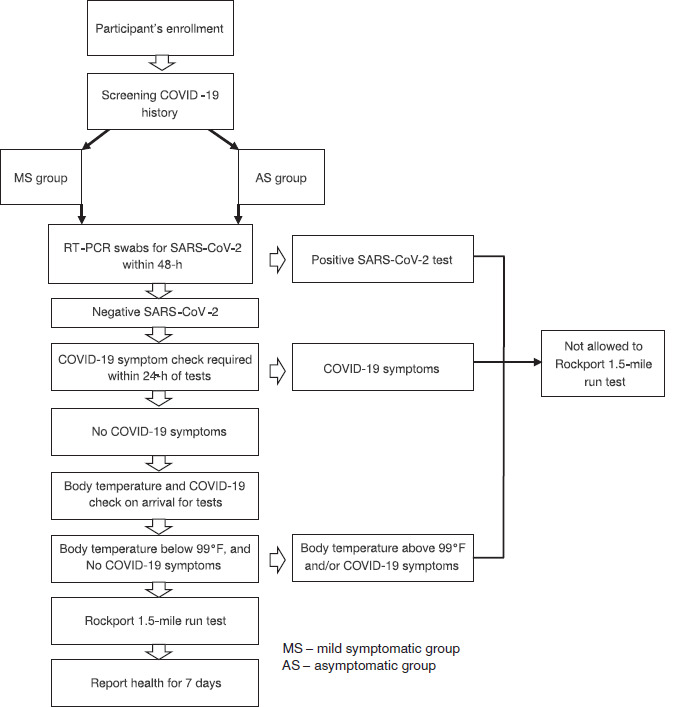
The participants for this study were recruited through posters that outlined the inclusion and exclusion criteria. They were required to provide a doctor’s certificate as evidence of them being a previous carrier of the disease. A week before the testing phase, a familiarisation session regarding the test implementation protocol was conducted. This study lasted for 10 days (1st – 10th october 2022), with 5 participants being tested in a day. The participants were divided into two categories, namely MS and AS groups, to receive the Rockport 1.5-mile run test.
Before conducting the Rockport 1.5-mile run test, each participant received anthropometric measurements indoors under the supervision of a male medical representative (n = 1) and an administrator (n = 1). Their body weight, body mass index (BMi), and fat, were measured using the omron digital Weight Scale HN 289, while Seca 214 Portable Stadiometer from Cardinal Health, ohio, USA, was applied for height measurements. Following this, the Rockport 1.5-mile run test was conducted every morning from 08.00 a.m. to 10.00 a.m. This was performed under specific weather conditions, including temperatures ranging from 24–27°C and relative humidity between 15–23%. during the test, heart rate (HR) was continuously monitored using a Polar V800 GPS. immediately after, the participants were asked to rate their perceived exertion (RPE) using the modified Borg’s CR10-scale, as described by Foster et al. [20]. Figure 1 presents the study design and clinical procedures.
Safety measures
This study was conducted in early 2022 when the status of the pandemic in indonesia had become endemic. However, the safety of both the patients and medical staff remained a top priority. Therefore, all testing staff in this personal study were required to comply with the protective equipment (PPE) guidelines set forth by the indonesian Ministry of Health. This included the use of an N95 mask, face shield, gown, and gloves during the testing process. Before conducting the test, the entire committee ensured that all equipment was properly sterilised by thoroughly disinfecting them with an appropriate spray.
All participants and testing staff were required to perform 2 consecutive negative RT-PCR swabs for SARS-CoV-2 at least 48 hours apart before the test began. during the Rock-port 1.5-mile test, the distance was set at 2 m between participants. Furthermore, drinking water ad libitum was allowed to maintain hydration. However, it was required that drinking bottles not be shared, and any damaged or worn-out pieces used were promptly replaced. Participants were instructed to immediately report to the medical staff when they experienced any symptoms suggestive of CoVid-19 within the following 7 days.
Physiological and RPE-BoRG scale measurements
Before the CRF level test, the blood pressure (BP) of each participant was measured using the omron Wrist Blood Pressure Monitor HEM-6181. CRF level was measured by applying the Rockport 1.5-mile run test, a method that was adopted by previous studies [21, 22]. The timing gate system (Smart Speed
Fusion, Australia) was employed at the start gate (point 0 meters) and finish gate (point 2,414 meters) to measure the time taken to complete the test. Participants were instructed to walk as fast as possible while keeping 1 foot in contact with the ground. To measure the final HR, a Polar V800 GPS was placed on the participant’s chest. immediately after the test, RPE values were determined using Borg’s CR10-scale RPE value. The divisions of the scale were 0, 1, 2, 3, 4, 5, 6–7, and 8–10, all indicating rest, very easy, easy, moderate, somewhat, hard, very hard, and maximum, respectively.
Statistical analysis
This study utilised iBM SPSS software, V.25.0, to perform statistical analysis tests. Specifically, the formula proposed by Kline et al. [23] was employed to estimate the Predicted Vo2max based on the 1-mile walk of each participant.
Vo2max = 132.853 − (0.0769 × WT) − (0.3877 × AGE) + (6.315 × SEX) − (3.2649 × TiME) – (0.1565 × HR)
where WT – weight (lb), SEX – males, 1 and females, 0, TiME – walking time (min), and HR – final heart rate (bpm). All data were tested for normal distribution using the Shapiro–Wilk test and Levene’s statistics. To examine differences in blood lactate and RPE variables, a one-way ANoVA with independent t-test was conducted. Confidence intervals (95% Ci) were calculated to indicate the magnitude of change, while statistical significance was determined at the p < 0.05 level.
Results
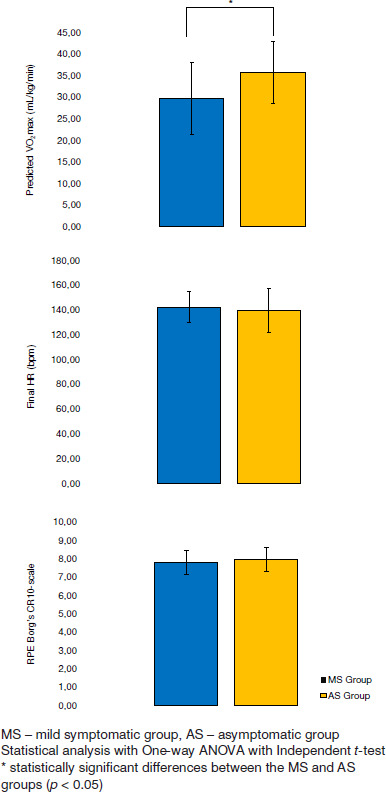
Table 1 provides a comparison of anthropometry and BP between the MS and AS groups. Table 2 and Table 3 show the percentage of symptoms observed in the MS group, and the corresponding mean time, respectively. Figure 2 presents differences in several variables, such as Vo2max, final HR, and RPE, between the MS and AS groups.
Table 1
Characteristics of participants, divided by groups
Table 2
Characteristics of symptom history in the MS group
| Symptom parameter | Percentage 100% (n = 25) |
|---|---|
| Rhinitis | 20% |
| Breathing problems | 40% |
| Headache | 92% |
| No sense of taste and/or smell | 88% |
| Chest pain | 44% |
| Sore throat | 40% |
| Cough | 80% |
| Sniffles | 68% |
| Listlessness | 72% |
| Aching limbs | 96% |
Table 3
Time taken to perform the Rockport 1.5-mile run test
| Variable | MS group (mean ± SD) | AS group (mean ± SD) | p-value | Effect size |
|---|---|---|---|---|
| Time (min) | 17.3 ± 1.9 | 15.5 ± 1.2 | 0.001* | 0.262 |
The results of anthropometry analysis showed that there were no significant differences between the two groups.
Similarly, during the Rockport 1.5-mile run test, the ANoVA indicated no significant differences in RPE (p = 0.396, ES = 0.015) and HR (p = 0.563, ES = 0.007) variables. However, differences were observed in the duration of the Rockport 1.5-mile run test (p = 0.001, ES = 0.262). These were followed by the Vo2max results (p = 0.007, ES = 0.140), which indicated a higher level of fitness in the AS group.
Discussion
The primary result of this study indicated that asymptomatic subjects, particularly males, have the highest Vo2max value, surpassing those who are healthy. This is indicative of a high CRF level [6], which is related to the normal/optimal functioning of the immune system [7, 8]. These support the study of Le Bert et al. [24], that asymptomatic individuals have mounted a highly functional virus-specific cellular immune response. Additionally, the conclusions of Long et al. [25] that asymptomatic individuals have a weaker immune response to SARS-CoV-2 infection, were refuted.
CRF is an indicator in determining the risk level for developing certain diseases [26, 27]. Specifically, it is often implemented in Vo2max calculations, and is a special attraction for study analysts as a focal point for investigation [28]. The primary objective was to establish a reference value of Vo2max within a given population, enabling the determination of health status [28–32]. For example, Sloan et al. [28] conducted a study involving 100 participants, employing the non-exercise fitness assessment (NEFA) method to measure Vo2max. The results showed values of 35.2 ± 5.0 ml/kg/min and 26.9 ± 4.6 ml/kg/min, for males and females, which indicated the standard for a healthy category within the Singaporean population.
Lee et al. [29], on the other hand, specifically stated that a low CRF can increase the risk of CV disease, type 2 diabetes mellitus, cancer, poor mental health, falls, and premature death. Therefore, it was recommended that measures, such as exercise, be conducted to increase this index [28, 29]. Previous studies, including Sloth et al. [30], indicated that performing sports three times a week can increase Vo2max. Specifically, it was stated that exercise with an intensity of 60–80% of HRmax is effective in increasing the level of CRF. This statement is essential, as it aligns with other literature, such as the World Health organization [26, 31].
This study represents the first attempt to measure the fitness level of CoVid-19 patients with MS and asymptomatic conditions using the Rockport 1.5-mile run test. The selection of this test was based on its endorsement in previous studies as the safest fitness assessment [33]. This study provides quantitative evidence supporting previous observations that CoVid-19 patients had a better fitness level. For example, Severa et al. [34] showed that asymptomatic patients have good immune resistance, explaining their lack of symptoms despite being infected. According to the results of this study, it appears that good immunity is produced by the presence of a high CRF level [19, 34].
This study, which was conducted in 2022, encouraged individuals to prioritise and enhance their CRF levels through regular exercise. Furthermore, it is believed to increase overall immunity, thereby reducing the risk of contracting CoVid-19. However, the results support previous studies that by increasing immunity through exercise, the risk of contracting various diseases can be lower. Additionally, a study conducted by Ramania et al. [35] serves as a valuable reference for sports enthusiasts, emphasising the significance of enjoying physical activities while benefiting from positive social interactions and supportive environments. Such factors contribute to reduced cortisol levels and enhance the effectiveness of sports engagement.
The several limitations of this study include the limited size and sex distribution of CoVid-19 samples that meet the criteria for this study, as they have to fit the number of patients under isolation on the day of data collection. The substantial number of asymptomatic patients, who are allowed to be discharged when the second swab test is negative, poses a challenge in recruiting an adequate sample size. Furthermore, it was realised that other factors, such as nutrition, psychology, and the circadian cycle of the participants, have not been thoroughly reviewed. Therefore, further studies are required to address aspects that have not been investigated.
Conclusions
Asymptomatic patients performed the Rockport 1.5-mile better than mildly symptomatic patients indicating asymptomatic patients had a higher Vo2max level than mildly symptomatic patients. Therefore, moderate-intensity exercise is recommended to increase CRF, thereby enhancing immunity and reducing the risk of contracting CoVid-19. This study encourages people to adopt a healthy lifestyle by paying attention to the CRF level as an indicator of healthy behaviour.