Introduction
Headache, a common and universal ailment, is a term that encompasses a spectrum of pain experienced in the head or neck region. Headache, a highly prevalent symptom, contributes to the most common nervous system disorders, collectively affecting 48.9% of the general population [1, 2]. Headaches are broadly classified into primary and secondary categories. Collectively, they account for approximately 20% of lost workdays globally [3]. The economic burden is estimated in terms of direct (cost of treatment and travel) and indirect (loss of productivity) costs [3].
Primary headaches, such as migraines and tension-type headaches, are common, but secondary headaches, particularly cervicogenic headaches (CGH), are also significant. Approximately 47% of the global population experiences headaches, with 15–20% of these being CGH [4]. These headaches stem from upper cervical spine dysfunction, typically causing unilateral pain that starts at the back of the head and neck, moves forward, and is often linked to restricted neck movement and arm discomfort [5, 6]. Neck-related disorders contribute significantly to societal burdens, reducing work capacity and productivity, making CGH a critical issue [6].
Researchers have highlighted the presence of fascial tissue known as myodural bridges, originating from the rectus capitis posterior major/minor and obliquus capitis, situated between the C1 and C2 vertebrae [6, 7]. These myodural bridges serve as structural connections linking suboccipital muscles to the dural tube. The proposed purpose of these bridges is to protect the cervical dura during movement, preventing compression of the spinal cord [6–9]. Under usual circumstances, when there is no tension or headache, the dural tube has a minor movement of folding inward, and the myodural bridge plays a role in facilitating this folding process, which is required for the smooth sliding of the dural [7]. This reinforces the significance of the myodural bridge, as it creates a direct anatomical connection between the muscles, cervical fascia, and dural tube [7–9]. Recognising muscular dysfunction as a potential contributing factor to CGH suggests a potential impact on the myodural bridge, influencing the folding of the dural tube around the spinal cord. The imbalance of suboccipital muscles can result in sustained neural tension along the myodural bridge. Considering the high sensitivity of the dural tube, any abnormal tension within it may play a role in triggering CGH [7]. Structural alterations in the cervical musculature, particularly the suboccipital muscles, have been increasingly recognised in individuals with cervicogenic headache. These deep neck muscles play a key role in sensorimotor control and stabilisation of the upper cervical spine. There is supporting literature that has demonstrated that individuals with CGH, particularly older women, exhibit significant atrophy and structural changes in the sub-occipital muscles compared to controls. Such findings support the clinical relevance of evaluating suboccipital muscle thickness, as it may reflect underlying neuromuscular dys-function contributing to headache symptoms. Including this parameter as an outcome measure may offer insights into the morphological adaptations associated with CGH and help guide targeted interventions [10].
Conventional management, like pharmaceutical drugs, is regularly used in treating CGH and to reduce the intensity and frequency of this headache. NSAIDs, including ibuprofen and ketoprofen, are commonly used in the treatment of CGH [11]. Any medications taken excessively and taken over the counter without a proper prescription are prone to have severe side effects like gastrointestinal ulceration or bleeding due to consuming excessive NSAIDs. Opioid analgesics commonly cause constipation, addiction or dependence, drowsiness, dizziness, etc. [11].
Physiotherapy has the advantage of being a safe and effective alternative to medication. Recent updated clinical practice guidelines on the management of CGH support the use of exercise therapy, manual mobilisation and spinal manipulation to reduce CGH pain intensity, frequency and disability [12, 13]. Although there is supporting evidence that spinal manipulation significantly reduces symptoms in individuals with cervicogenic headache, there is also evidence which suggests that experts may prefer not to use spinal manipulation for CGH because of the risk of adverse events, which have been frequently mentioned in the literature. As a result, various manual mobilisation techniques are often preferred in CGH management [13].
Mulligan’s concept, referred to as mobilisation with movement, possesses unique features that distinguishes it from other manual mobilisation approaches, one of which is that it integrates manual mobilisation techniques with active movement [14]. Within the Mulligan concept, sustained natural apophyseal glides (SNAG) represent a technique wherein a painless joint glide is applied while the patient actively performs the movement [14, 15]. Various systematic reviews favour the use of sustained natural apophyseal glides (SNAGs) as part of non-pharmacological management of cervicogenic headache [14–18]. The clinical practice guidelines suggest that SNAGs and low-load cervical exercises can be considered a standard line of management for cervicogenic headache [13, 19–22]. The use of exercise therapy as a conservative management approach for cervicogenic headache (CGH) is well-supported in the literature, particularly focusing on low-load craniocervical and cranioscapular exercises [13, 19–21]. The emphasis on low-load exercises is important in preventing exacerbation of symptoms and ensuring the safety of individuals with CGH. Integrating these exercises into a comprehensive treatment plan under the guidance of a qualified physiotherapist can contribute to reducing symptoms and improving functional outcomes. However, the potential effect of SNAGS and low-load exercises on cervical muscle dysfunction visualised based on cervical muscle thickness in relation to the myodural bridge or dura using ultrasonography is seldom studied, and there is a lack of supporting evidence considering the carryover effects of these techniques on the clinical metrics of cervicogenic headache.
Recent physiotherapeutic approaches emphasise the fascial concept for managing various neuro-musculoskeletal conditions [23]. This concept characterises the fascia as the most extensive and interconnected tissue in the body, forming a comprehensive three-dimensional network that spans from head to toe. Fascia can be targeted using myofascial release techniques, constituting a powerful approach for treating soft tissue dysfunction [23–26]. The application of myofascial release (MFR) techniques, such as trigger point therapy and suboccipital release, in reducing the intensity of CGH has been researched with positive outcomes [23–26]. However, none of these techniques targeted the dural tube as a potential factor for CGH, which would have an impact on the muscle thickness connecting the dural tube, as one of the rationales for CGH is dysfunction in the anatomical connection between the muscles, cervical fascia and dural tube. A myofascial release technique in the form of dural tube myofascial release targeting these structures can be considered as a choice of treatment in CGH [23]. Though less is known about this technique, there is supporting literature on the positive effects of myofascial release in the form of trigger point and suboccipital release on reducing the intensity of CGH. Thus, it was hypothesised to determine and compare the effect of dural tube myofascial release with sham release along with standard physical therapy care on suboccipital muscle thickness, cervical flexion-rotation range, and the clinical metric of headache in individuals with cervicogenic headache.
Subjects and methods
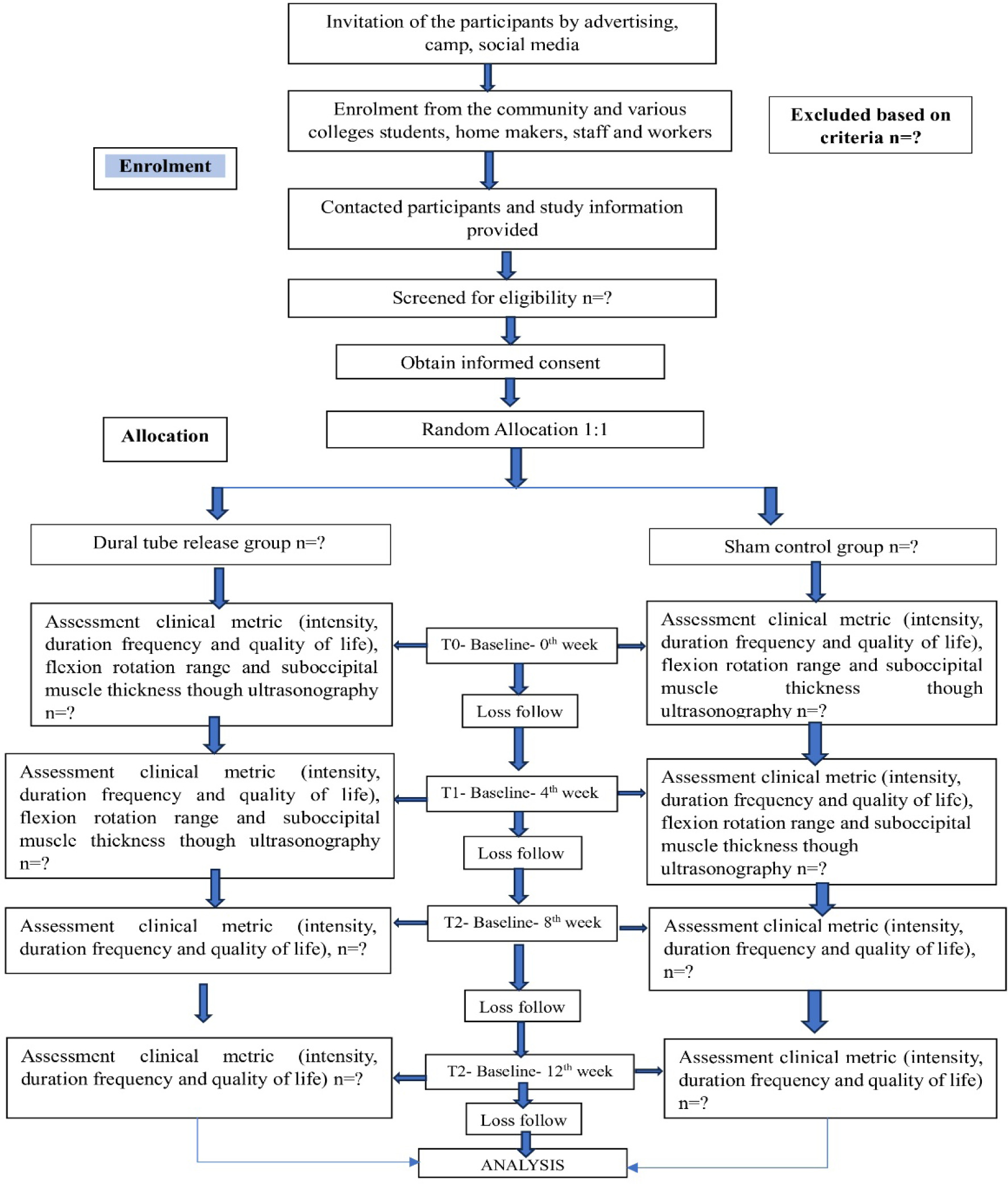
The research protocol was established in accordance with the SPIRIT (Standard Protocol Items Recommendations for Interventional Trials) reporting guidelines for protocol studies [27] and is registered in the Clinical Trials Registry of India under CTRI/2024/11/077197. To ensure comprehensive reporting and transparency throughout the trial, the CONSORT- 2010 Statement: Extension to Pilot Studies and Feasibility Trials guidelines have also been referenced (Figure 1). These guidelines are utilised to enhance the clarity, consistency, and quality of the study’s design, ensuring that all necessary elements of the protocol are adequately described and that the trial’s procedures are aligned with established best practices for pilot and feasibility research.
Trial design
This is an open-label, randomised, parallel-armed, assessor-blinded controlled trial. Participants will be randomly assigned to one of two study groups using block randomisation, based on a computer-generated random number table. The randomisation process will be performed by a statistician who remains blinded to the intervention groups. The trial will be conducted at a tertiary care centre located in Belagavi city.
Participants
The participants will be individuals aged 18–50 years who have been diagnosed with CGH and meet the following criteria: a confirmed diagnosis of CGH based on the cervicogenic headache international study group (CHISG) [12], with the presence of unilateral head pain that does not shift sides and is accompanied by neck pain. Participants must also exhibit a positive flexion-rotation test result of less than 33 degrees [12]. Participants should also be willing to engage in the intervention and commit to follow-up for 12 weeks. Participants will be excluded if they meet any of the following criteria: a primary headache diagnosis according to international classification of headache disorders (ICHD-3) [5], presence of any red flags for manual therapy [13] (such as spinal infection, vertebral tumours or fractures, cervical instability, metabolic diseases, rheumatoid arthritis, osteoporosis), symptoms of dizziness or visual disturbances, inflammatory skin conditions, ulcers or wounds in the treatment area, or any medical or surgical conditions that prevent the participant from assuming a prone position (required for the intervention). The exclusion criteria also include the use of prescribed analgesics, physiotherapy, or any other allied therapies for headache, cervical pain, or related conditions within the past month, radiating pain or neurological deficits in the upper extremities, known cervical disc conditions, cervical spine arthritis, a history of central nervous system involvement, vestibular dysfunction, prior head or neck surgery, and pregnancy.
Recruitment
The recruitment of CGH participants will be systematically organised through a combination of strategies, including community-based screening camps in various neighbour-hoods and screenings at a tertiary care hospital. Prior to the start of these camps, a comprehensive awareness campaign will be launched, utilising multiple platforms such as flyers, pamphlets, regional newspaper advertisements, and social media to inform the public about the musculoskeletal and headache screening and treatment camps. The campaign will highlight the benefits of early detection and diagnosis, aiming to encourage greater participation. Participants will be invited to join the study through these outreach efforts. Interested individuals will then be screened for eligibility, and a detailed explanation of the study will be provided to them before enrolment.
Randomisation
Eligible participants who provide informed consent will be randomly assigned to one of two groups: the dural tube release group or the sham group. Randomisation will be carried out using a block randomisation method, ensuring that participants are distributed evenly between the two groups. This process will involve a computer-generated random number table to assign participants in a 1:1 ratio. The block randomisation technique will help to maintain balance between the groups throughout the enrolment process, ensuring that the number of participants in each group remains equal, reducing the risk of bias. This approach will allow for a fair comparison of the effects of the dural tube release intervention versus the sham procedure.
Blinding
This study will be conducted as a double-blind controlled trial, meaning that both the participants and study personnel involved in the treatment or assessment process will be unaware of the group assignments. To ensure objectivity and eliminate bias, an independent assessor and a statistical data analyst will be blinded to the identity of the groups. The participants will be randomly assigned to either the dural tube release or sham group, but the groups will be coded as group A and group B, with the actual treatments concealed from both the assessor and the analyst. This blinding process will help maintain the integrity of the data and ensure that the outcomes are assessed impartially, free from any influence of group allocation.
Study intervention
To ensure the quality and consistency of intervention reporting, the study will adhere to the Template for Intervention Description and Replication (TiDieR) and the Consensus on Exercise Reporting Template (CERT) guidelines/checklists [28, 29]. Prior to participation, selected participants will be fully informed about the study in their vernacular language, including details about the study procedure, potential risks, risk management strategies, and the benefits of participation. A written informed consent form will be obtained from all willing participants, and a copy of the consent form will be provided to them for future reference. Demographic information will be collected, and the participants will undergo an orientation session before the intervention begins. During this session, they will be thoroughly briefed on the study protocol to ensure their full understanding.
Description of intervention
The intervention will be given by a trained physiotherapist and a certified manual therapy practitioner.
Common intervention
The experimental and control groups will receive a common intervention consisting of sustained natural apophyseal glides (SNAGs) and low-load exercises. The SNAG techniques [18] will be given for 6 repetitions and the glide will be sustained for 30 s. These SNAG techniques will be modified for participants with or without headache and based on the comfort of the participants. The details are presented in Table 1. Low-load exercises include cervical flexion loading exercise, scapula retraction exercise, neck isometrics, and neck mobility exercises [18, 23]. In the initial four weeks, the participants will perform 2 sets of 10 repetitions with a 10-second hold and 10 s of rest. The details of the exercises and progression are presented in Table 1. At the end of the fourth week, the participants will be advised to independently continue similar exercises at home once daily up to 12 weeks. The intensity of the exercise for the home exercise program will gradually progress to 3 sets of 10 repetitions with a 10-second hold over the next 4 weeks (up to 8 weeks) and in the next 4 weeks (up to 12 weeks), the intensity will progress to 3 sets of 15 repetitions with a 15-second hold.
Table 1
Description of common intervention and dosage given to both groups
Experimental group (dural tube myofascial release + SNAGs + low-load exercises)
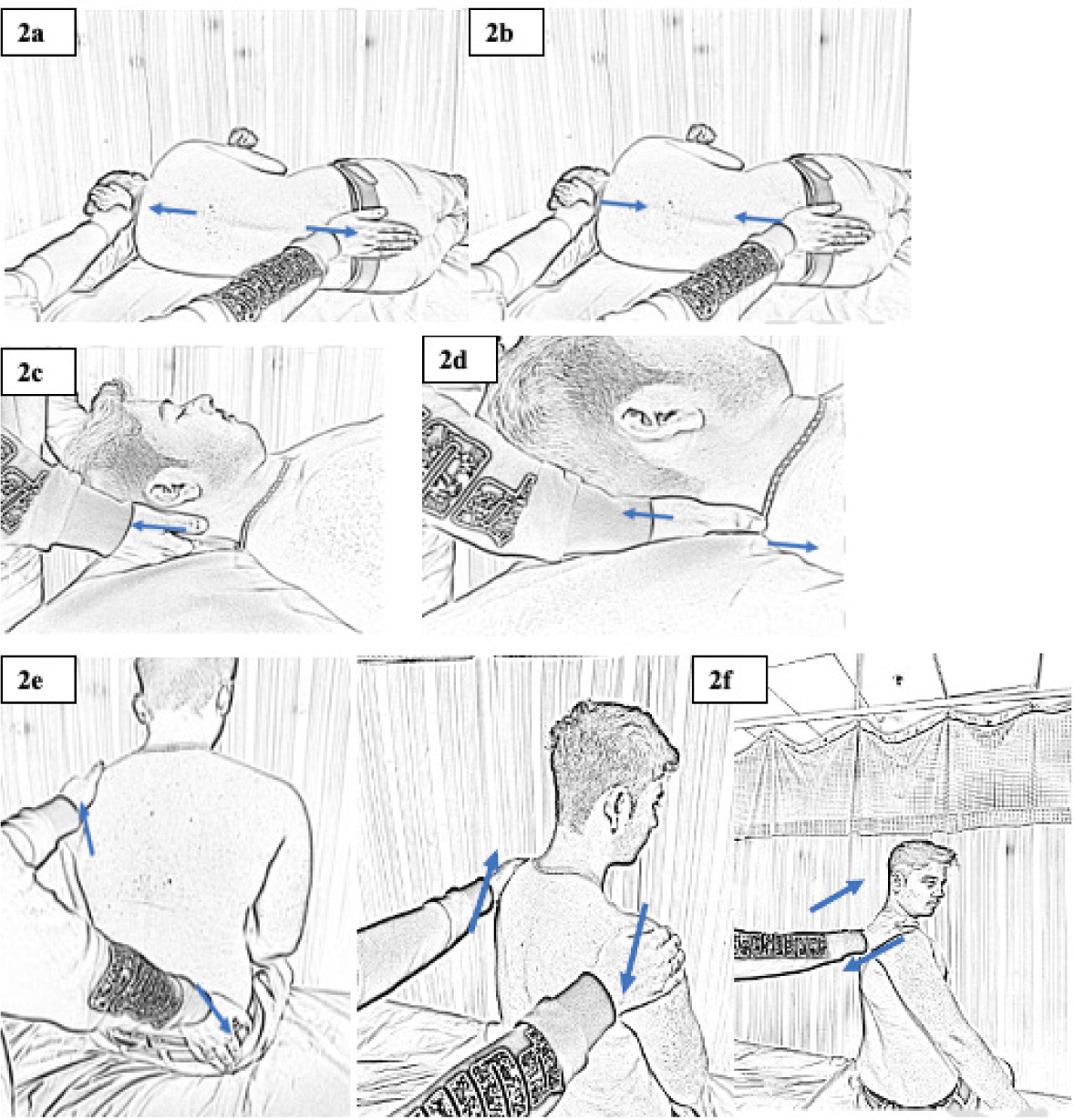
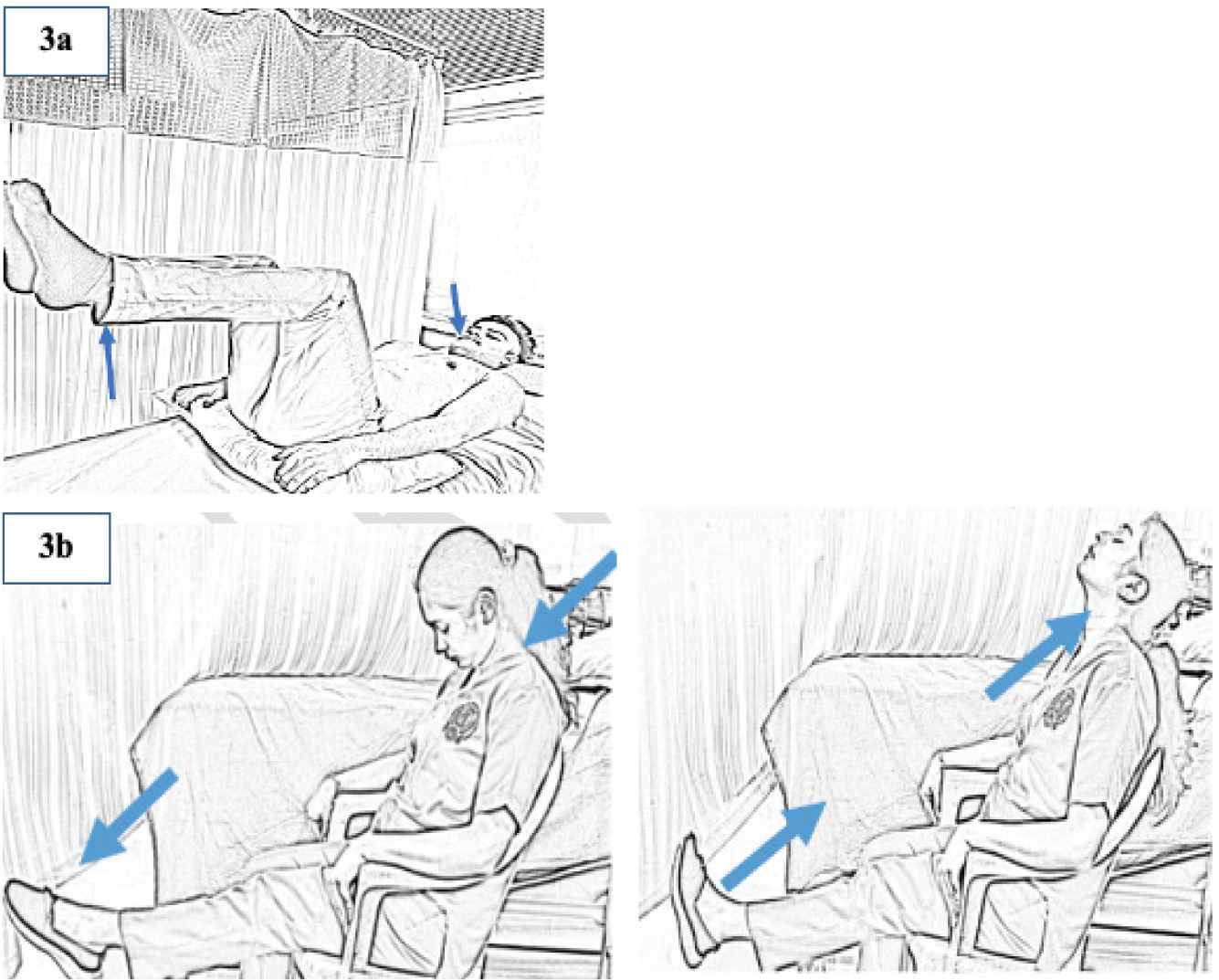
Along with the common intervention, the participants in this group will receive myofascial dural tube release, comprising a combination of dural tube stretch and compression, gross posterior cervical release, three-dimensional release, and self-stretch for dural tube release [30]. Table 2, Figure 2(a–f), and Figure 3(a–b) outline the specifics of the dural tube release protocol. Each technique will be administered with three repetitions, sustained for 30 s each. After the fourth week, participants will be instructed to continue the self-dural tube stretch once daily up to 12 weeks.
Table 2
Description of intervention and dosage given to dural tube release group
Control group (sham dural tube myofascial release + SNAGs + low-load exercises)
Along with the common intervention, this group will receive sham dural tube myofascial release techniques, involving only contact with the hand will be maintained. Each technique will consist of three repetitions, sustained for 30 s each.
Duration of treatment and dosage
Participants will undergo the intervention for 40 min three times a week on alternate days for a duration of four weeks. On the days when there is no treatment, they will be asked to do the home exercises (low-load exercises). At the end of the 4th week, they will be encouraged to continue a home exercise program consisting of low-load exercises up to 12 weeks.
Adherence to intervention
Compliance with the home exercise program will be monitored by providing the participants with a logbook or diary that includes the prescribed exercises, along with the required number of sets and repetitions. At the conclusion of the 4-week intervention period, the participants will be instructed to continue the exercises for an additional 8 weeks, extending the total duration to 12 weeks of intervention. To support adherence, regular telephone reminders will be provided throughout the follow-up period.
Criteria for dropout
Participants will be excluded from the study if they experience any adverse events related to the home exercise program or intervention. Those who do not adhere to the intervention protocol, defined as participating in less than 70% of the prescribed intervention days during the initial 4-week period, will also be considered for dropout. Participants who complete fewer than 50% of the home exercise sessions will also be excluded. However, those who miss one or both follow-up assessments at the 8th and 12th weeks will be included in the intention-to-treat analysis and will not be considered dropouts.
Criteria for protocol modifications/discontinuation
The protocol will be modified only if adverse events occur or if practical challenges arise during the trial. Any changes will be submitted to the Research Ethics Committee for approval.
Data collection procedure
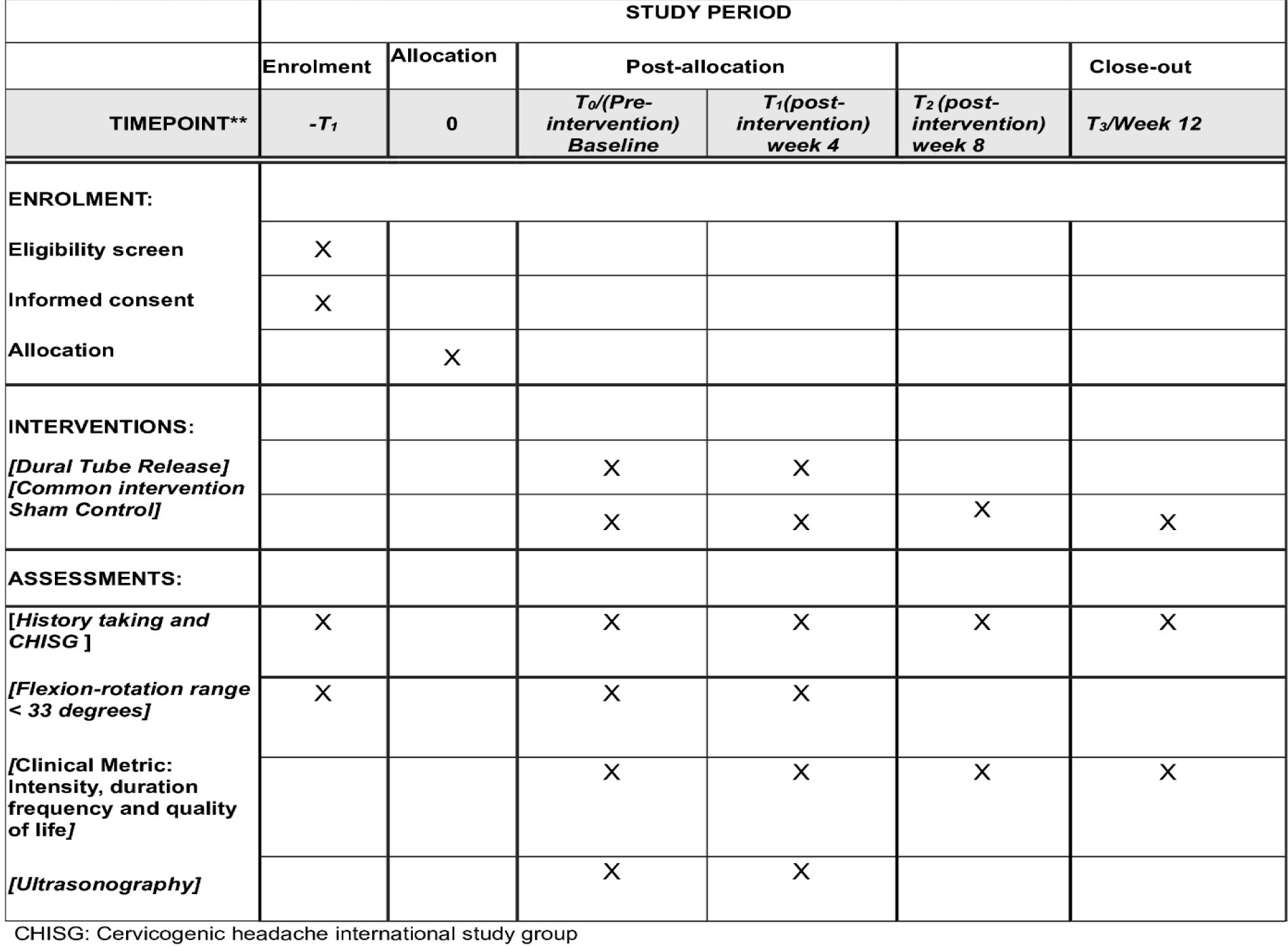
The outcome assessments will be carried out by a qualified physiotherapist who will be blinded to the group allocation. Suboccipital muscle thickness assessment using ultrasonography and flexion-rotation range assessed using a digital goniometer will be assessed at baseline and after four weeks. Intensity, frequency, duration and quality of life will be assessed at four time points: pre-treatment (T0) and at the end of the fourth week (T1), eighth week (T2) and twelfth week (T3) follow-ups (Figure 4).
Figure 4
Schematic diagram of schedule of enrolments, intervention’s and assessment (participant timeline)
Assessment of the clinical metrics that include intensity, duration, frequency, and quality of life: Headache intensity will be measured on a scale from 0 to 25 (from ‘no pain’ to ‘worst possible pain’) [31]. Frequency will be recorded in terms of days per week or month [31]. Duration will be assessed based on how long each headache episode lasts, ranging from minutes to hours [31]. Quality of life will be evaluated using the 25-item Headache Disability Index (HDI), which measures the emotional and functional impact of headaches. Scoring ranges from 0 (No) to 4 (Yes), with a total score between 0 and 100, where higher scores indicate greater disability [32]. The HDI has proven reliability and is simple for patients to complete and interpret, providing valuable insight into how headaches affect daily life. The HDI will be given in English during the recruitment; we will check their language ability through a short conversation to make sure they can understand the questions. If any participant needs help in understanding a question, we will explain it without affecting their answers. If needed, we will provide a translated version of the questionnaire in the local language, depending on the participant’s language background. All the clinical metrics are self-administered and are reported by the patient.
Suboccipital muscle thickness assessment using ultra-sonography: This will be done by a qualified radiologist. The suboccipital muscle thickness will be assessed for all participants recruited in the study. The muscles that will be assessed include the rectus capitis posterior and obliquus capitis muscles. Each suboccipital muscle thickness will be marked by the radiologist using the software installed in the system by application of digital tools (line, point, ruler, and circle). The reference points included for marking on the radiographs will be as per the reference article [33].
Flexion rotation range assessment: This will be measured using a digital goniometer. With the patient in supine position, the head and neck will be positioned into maximum flexion and rotated to either side until the onset of pain or the maximum range at which firm resistance was reached. Range of motion will be monitored for rotation of the cervical spine on the right and left sides [34].
Sample size
The sample size was determined using clinical metrics of headache outcome from a prior study [19]. The expected mean difference (x1–x2) was assumed as 12 = d. The SD values were S1 = 15.76 (SNAGs group) and S2 = 6.09 (Exercise group). The following formula was used using the values and assumptions that were available:
where: S = S1 + S2/2 = 10.92
Z1–α = 2.58 at 1% error or 99% confidence
Z1–β = 1.6820 at 5% error or 95% power
d = x1–x2 = 12
As a result, the sample size was determined to be 30 per group. Using the formula n/1–d, where d is the percentage dropout rate, and accounting for a 10% dropout rate, the net total sample produced 34 individuals in each research group, for a total of 68 participants.
Safety monitoring
Participants will be required to obtain fitness approval from their family physician before participating in the study. The anticipated risks are minimal and primarily involve mild discomfort or muscle soreness due to the manual therapy and exercise interventions, which are typically self-limiting. To minimise these effects, rest intervals will be adequate, and exercise intensity will be gradually increased. In the event of more severe adverse events, such as dizziness, worsening of headache, vertigo, nausea, vomiting, light-headedness, or blurred vision following the intervention, the ethical review committee will be promptly notified. The affected participant will be withdrawn from the study and referred for further evaluation and care.
Data management
An Excel spreadsheet will be used to manually enter data, guaranteeing participant privacy. Only the lead investigator will have access to the safely kept records. The statistician will remain blinded by designating the intervention groups as A and B. Data about participants will be coded and not disclosed without de-identifying them.
Statistical methods
IBM SPSS (Statistical Package for the Social Sciences) software version 28 (Chicago, IL, USA) will be used for statistical analysis. The data will be subjected to both descriptive and inferential statistics. Standard deviations and means will be used to express quantitative variables. The following tests will be performed: independent t-tests or Mann-Whitney U tests for between-group comparisons, dependent t-tests or Wilcoxon matched pairs tests for within-group comparisons, and repeated measures ANOVA for time vs. group interaction. The intention-to-treat principle will guide the primary analysis, and a p-value of less than 0.05 will be considered statistically significant.
Confidentiality
Every participant’s information collected for this study will be kept private. Coded group data will be used in presentations and publications for scientific purposes. Password-protected electronic storage will be used to store the data. The authors will take the necessary precautions to protect the participants’ identity, including hiding them in any published photos, and will make sure that their names are not revealed.
Discussion
Headaches have affected nearly 95% of the general population at some point of life, with an annual prevalence approaching one in two adults [2]. Acknowledging the significant burden they impose, the World Health Organization classifies headaches among the top 10 causes of disability [35]. These enervating headaches significantly diminish an individual’s quality of life, resulting in substantial healthcare costs and broader economic consequences indirectly [2, 3, 35].
Cervicogenic headache (CGH) is commonly linked to physical impairments in the joints, muscles, and neural structures of the cervical region, particularly the upper spine. Due to the referral of pain from the neck, CGH is frequently misdiagnosed and overlooked in individuals experiencing neck pain, leading to inadequate treatment [4, 6]. The prevalence rate of CGH in India has been studied in various occupations and working-age groups from 18 to 50 years old. Reported prevalence rates include 27.14% among hospital nurses [36], 15% among dentists [37], and 34.85% among computer users [38]. In clinical practice, it is common to come across conditions that are prevalent and regularly treated, yet they face limitations in research and a lack of consensus among experts. CGH is an example of such a condition [5, 35]. Only within the last two decades has this subject gained attention in the mainstream of headache and pain literature [5].
A potential rationale for CGH is that a cervical muscle imbalance leads to tension being transferred to the dura via the myodural bridge, which results in an increase in the frequency of CGH [6, 7]. There is supporting evidence that there is a fascial tissue known as the myodural bridge that connects the neck muscles (rectus capitis posterior and obliquus capitis) to the protective covering of the spinal cord, known as the dural tube [6–9]. This connection between the suboccipital muscles and the myodural bridge that is connected to the dura has been researched and confirmed through cadaveric studies using MRI [39] and USG [33] based evaluation of the structures.
Physical therapy in the form of manual therapy and exercise therapy is considered safe and effective [13]. Supporting literature suggests the beneficial effect of SNAGs in the management of cervicogenic headache [14–16, 25, 40, 41]. The clinical practice guideline for CGH, formed through literature research and grounded in high-quality evidence, puts forth recommendations indicating that low-load craniocervical and cervicoscapular endurance exercises, along with manual therapy, is effective in managing CGH [13, 19–21].
Scientifically conducted randomised clinical trials and controlled trials have provided substantial evidence supporting the effectiveness of low-load exercises, defined as exercises that involve minimal muscular activation without external resistance, primarily targeting deep cervical stabilising muscles in the craniocervical and cranioscapular regions, which is proven to be effective in reducing both the intensity and duration of CGH [15, 19–21, 40]. Moreover, favourable outcomes were observed when these exercises were combined with cervical mobilisation [15, 20, 21]. These exercises aim to enhance muscle control, stability, and flexibility without causing undue strain on the cervical and cranioscapular structures [19–21]. The literature strongly supports the use of low-load craniocervical and cranioscapular exercises as a conservative and effective management strategy for individuals experiencing CGH [19–21]. The outcomes of the study will help us confirm the effect of the standard physical therapy care through objective outcomes using ultrasonography on suboccipital muscle thickness and the flexion-rotation test.
Existing literature provides strong evidence supporting the positive impact of myofascial release techniques, such as trigger point therapy and suboccipital release, in alleviating the intensity of CGH [23, 25, 26]. These approaches have been shown to reduce pain and improve function for individuals suffering from CGH. Since the underlying pathophysiology of CGH points to dysfunction in the anatomical relationship between the muscles, cervical fascia, and the dural tube, applying myofascial release techniques that target these specific structures, especially through dural tube myofascial release, emerges as a promising treatment approach. The sub-occipital muscles, which coordinate upper cervical rotation, are often affected in CGH. Studies support the reliability of ultrasound in measuring the thickness of these muscles and link greater muscle thickness to improved cervical stability and mobility in CGH patients [33]. In addition, the myodural bridge connective tissue linking the suboccipital muscles to the dural tube serves as a structural pathway for transmitting tension [9]. Am imbalance in suboccipital muscles may lead to prolonged neural tension through this bridge, potentially contributing to CGH symptoms [8, 9].
Several review articles suggest that abnormal tension in the dura mater could contribute to the development of CGH, this theory is supported by the concept of the myodural bridge, a fascial connection that links the craniocervical muscles to the dura mater, which acts as the protective covering of the spinal cord, this anatomical connection may play a significant role in the onset of CGH, and techniques that address this dysfunction could offer substantial therapeutic benefits [6–9]. Dural tube release and self-dural stretching specifically target the myodural bridge – a connective tissue connection between the suboccipital muscles and the spinal dura mater. This area is important because tension here can affect nerves and contribute to headaches. Unlike craniocervical exercises, which mainly focus on strengthening and improving motor control, dural release techniques help reduce tightness and irritation around the dura itself. This can lead to less nerve irritation, thereby improving nociceptive inhibition and neuro-muscular control, allowing the suboccipital muscles to activate more effectively. This gives an advantage to the participants who undergo dural release in terms of better motor unit activation, muscle recruitment, and stronger contraction with low-load exercise stimuli. Thus, while both groups perform the same low-load exercise, the group receiving dural tube release may exhibit a comparatively larger increase in thickness due to better muscle recruitment and reduced inhibition [6–9].
To the best of our knowledge, this is the first study to explore the impact of dural tube release on decreasing the pain intensity, frequency, and duration of headache, along with the increase in flexion-rotation range and suboccipital muscle thickness.
Limitations
The study has some limitations. While MRI would have been a more ideal method to assess myodural bridge thickness, the high cost of MRI prompted the use of ultrasonography to measure suboccipital muscle thickness, which is a reliable tool for evaluating this in CGH, as supported by existing literature [32]. However, maintaining consistent timing for follow-up ultrasonography assessments may pose practical challenges during data collection, potentially affecting the reliability of the measurements.
Expected outcome
The study outcomes will determine whether dural tube myofascial release offers additional benefits over standard physical therapy or if its effects are merely placebo in managing CGH. By using objective measures such as ultrasonography for suboccipital muscle thickness and the flexion-rotation test, the study will evaluate the impact of standard physical therapy care. The study will examine improvements in key clinical outcomes; these include increased muscle thickness, enhanced flexion-rotation range of motion, improvement in quality of life and reduction in headache frequency, intensity and duration of equal to or less than 50% compared to pre-intervention at follow-up. The findings will offer valuable insights into the long-term effectiveness and carry-over effects of physical therapy interventions for CGH. A positive result may support the integration of dural tube myofascial release into clinical practice guidelines, potentially decreasing the dependency on pharmacological treatments.