Introduction
Low back pain is one of the most common manifestations of musculoskeletal pain and has reached pandemic proportions in recent years, with nearly 10% of the global population experiencing lower back pain in 2020 alone [1]. in 2015, 7.3% of the world’s population experienced activity-limiting low back pain, indicating that approximately 540 million individuals were affected at any moment. Currently, low back pain stands as the primary cause of disability worldwide [2], and according to the 2020 Global Burden of Disease (GBD), around 619 million individuals were impacted worldwide. Projections suggest that this will rise to around 843 million cases by 2050, with the increase primarily attributed to population growth and ageing [3].
Chronic non-specific low back pain (CNLBP) is defined as pain and/or discomfort localised in the area between the lower ribs and the gluteal fold that has no known pathoana- tomical aetiology (such as a tumour, fracture, osteoporosis, or radiculopathy syndrome) and lasts longer than three months (i.e., beyond typical tissue healing time) [3, 4]. More than 90% of low back pain cases worldwide refer to a non-specific aetiology [5].
Clinical guidelines for CNLBP management recommend the application of manual therapy (MT) techniques (manual techniques and therapeutic exercises) combined with patient education and consultation, as well as maintenance of physical activity levels [6, 7].
Research has shown that MT reduces muscle spasms and pain and improves tissue mobility and range of motion [8]. However, the MT approach uses the biomedical model of pain, which suggests a dependent cause-and-effect relationship between pain intensity and tissue pathology and dysfunction [9]. On the other hand, chronic musculoskeletal pain does not always follow a cause-and-effect relationship regarding its origin since it is a complex condition involving physical, psychological, and socioeconomic factors [10]. Pain perception and intensity, as well as the resulting functional disability, are subjective and can be influenced by various elements related to the individual’s attitude and environment [11]. Catastro- phising personal beliefs and expectations and avoiding movement caused by pain are typical examples of such factors [12, 13].
For these reasons, patient education has been recently proposed as a method for managing chronic pain [9]. Pain neuroscience education (PNE) is a cognitive therapy and constitutes a top-down educational therapy [14, 15]. The objective of PNE is to explain to patients the neurobiological processes, the physiology of pain, nociplastic pain, Penfield’s homunculus, pain-related changes in body perception, and the psychosocial expression of the pain they experience in a way they can understand. To this end, metaphors, examples, and images modify perceptions, misinterpretations, and maladaptive thoughts associated with pain [16, 17]. Recent research has shown that PNE is an effective method for treating CNLBP, although its efficacy as a standalone therapy is still being debated [18].
It seems that combining MT and PNE can positively affect patients with CNLBP despite their contradictory nature (MT attributes the intensity of symptoms directly to tissue damage in the area, whereas PNE treats symptoms through central nervous system mechanisms) [9]. Based on the findings of a recent systematic review, PNE is an effective approach to improving pain, disability, and psychosocial factors in patients with CNLBP, especially when associated with other therapeutic regimens such as MT and exercises [19]. Similar findings were presented in a meta-analysis by Ma et al. [18], who indicated that adding PNE to treatment programmes (including MT and exercise) led to more efficacious results for CNLBP. Louw et al. [20] suggest that MT and exercise combined with PNE improve pain and disability, reduce psychosocial factors, promote active movement, and minimise healthcare utilisation. In any case, the exact effect of combining MT and PNE does not seem to have been sufficiently studied. The research question addressed in this narrative review was whether the combination of MT and PNE provided better results in CNLBP management than MT alone.
Subjects and methods
Search strategy
A narrative review was undertaken to investigate the effects of PNE in an MT intervention programme on improving the symptoms of individuals with CNLBP. Separate searches were conducted from November 1 to December 23, 2023. The PubMed, PEDro, and ScienceDirect databases were searched using combinations of keywords, including chronic low back pain, pain neuroscience education, pain neurophysiology education, and manual therapy. The database search also used two sets of Boolean operators:
Eligibility criteria
The inclusion criteria for articles were (1) participants with CNLBP, men and women (symptom duration of more than 12 weeks), (2) clinical trial study design involving at least two groups, with one group undergoing an MT intervention along with PNE, while the other group received the same MT intervention without PNE, and (3) articles published in the last 10 years (2013-2023). The exclusion criteria were (1) studies with a semi-experimental design (i.e., they were not randomised clinical trials), (2) articles not available in full-text, and (3) articles not published in English.
Data analysis
Data were analysed using a thematic synthesis approach, which involved identifying recurring themes and patterns related to the impact of PNE within MT intervention programmes for CNLBP symptoms. Qualitative and quantitative data were extracted and synthesised to provide a comprehensive understanding of the findings. Themes were developed based on the consistency and prevalence of data points across studies. The independent variable in this review was the type of intervention (MT alone vs MT with PNE), and the dependent variables included pain reduction, functional ability, and quality of life.
Study selection
Two authors independently reviewed the titles and abstracts derived from the different keyword combinations. They then attempted to retrieve the complete texts of the chosen articles and compared their findings. If an agreement could not be reached, a third reviewer was brought in to assist.
Results
The initial database search found 94 articles. After removing duplicates, 19 articles remained, and their titles and abstracts were reviewed based on the inclusion and exclusion criteria. Finally, five randomised clinical trials with a total sample of 248 adults were deemed eligible and included in the review. The study selection flow diagram is shown in Figure 1. The characteristics of each study are provided in detail below and comprehensively summarised in Table 1.
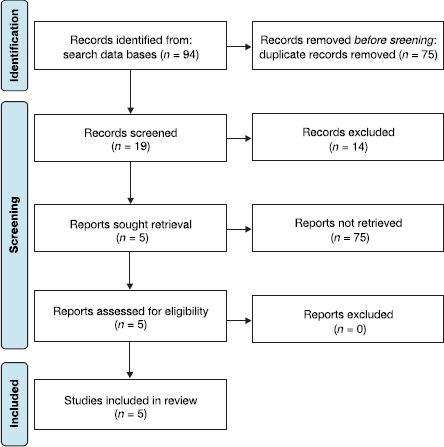
Table 1
Characteristics of the included studies
| Author and year | Number of participants | Intervention duration/ follow-up period | Intervention type | Outcome measures | Conclusions |
|---|---|---|---|---|---|
| Saracoglu et al. [14] | 69 | 4 weeks/3-month follow-up | intervention group 1: MT+ PNE + HEP Intervention group 2: MT + HEP Control group: Hep | NRPS Bps Odi Tsk | The combination of MT, PNE, and exercise produced the best short and medium-term results for improving back performance and reducing pain, disability, and kinesiophobia in individuals with CNLBP. |
| Tavares et al. [21] | 104 | 4 weeks/1-month, 3-month, 6-month follow-ups | group 1: Smt + PNE Group 2: Smt | NRPS Odi Gpe of improvement PSEQ Fabq | PNE plus SMT intervention had a significant medium-term effect of diminished pain intensity, as well as low back pain disability 3 and 6 months post-intervention. |
| Saracoglu et al. [22] | 35 | 4 weeks | group 1: Mt + PNE Group 2: Mt | NRPS Sf-36 | The combination of MT and PNE was more effective in reducing pain and improving the quality of life of people with CNLBP. |
| Song et al. [15] | 28 | 4 weeks/6- week, 8-week follow-ups | group 1: Stm +PNE Group 2: Stm | NRPS Csi Ppt Pcs Tsk-17 Rmdq | STM plus PNE may improve pain, pain cognition, and disability in patients with Cnlbp with central sensitisation compared to STM alone. |
| Tellez- Garcia et al. [23] | 12 | 3 weeks | group 1: Trp-DN Group 2: Trp-DN + PNE | RMDQ Odi Nrps Tsk Ppt | TrP-DN improved short-term pain, disability, kinesiophobia, and widespread pressure sensitivity in patients with mechanical LBP. The inclusion of a neuroscience educational programme only resulted in greater improvement in kinesiophobia. |
[i] Bps - Back Performance Scale, CSI - Central Sensitisation Inventory, FABQ - Fear Avoidance Beliefs Questionnaire, GPE - global perceived effect, HEP - home exercise programme, MT - manual therapy, NPRS - Numeric Pain Rating Scale, ODI - Oswestry disability index, PCS - Pain Cata- strophising Scale, PNE - pain neuroscience education, PPT - pressure pain threshold, PSEQ - Pain Self-Efficacy Questionnaire, RMDQ - Roland Morris Disability Questionnaire, SF-36 - Short Form-36, SMT - spinal manipulation therapy, STM - soft-tissue mobilisation, TrP-DN - trigger point dry needling, TSK - Tampa Scale for Kinesiophobia
Synthesis of results
Saracoglu et al. [14] focused on the efficacy of PNE in an MT and exercise programme in CNLBP patients in terms of pain intensity, back performance, disability, and kinesiopho- bia. Their primary hypothesis was that adding PNE to an MT programme would have better results compared to MT alone. The randomised clinical trial involved 69 patients randomly assigned to three groups (two interventions and one control). Group 1 followed a combination protocol that included eight MT treatments (mobilisation and manipulation techniques in the lumbar region) over four weeks (two sessions per week), with a session time of 45 min. PNE participants received training on how pain intensity is affected by perceptions and thoughts (one treatment per week lasting 40-45 min) and home exercises. Group 2 followed the same MT and home exercise programme without the application of PNE, while group 3 followed only the home exercise programme. The Numeric Pain Rating Scale (NPRS), Back Performance Scale (BPS), Oswestry Disability Index (ODI), and Tampa Scale for Kinesiophobia (TSK) were evaluated at baseline and after four weeks, with a follow-up 12 weeks after the end of the intervention. Results showed that participants in group 1 exhibited greater improvement in pain intensity and kinesiophobia compared to participants in group 2 and the control group on the fourth week (p < 0.05). Differences were also found for group 1 and group 2 compared to the control (p < 0.05). All differences remained statistically significant at the 12-week follow-up (p < 0.05). The study showed that combining MT, PNE, and exercise provided the best short and medium-term benefits in terms of improving back performance and reducing pain, disability, and kinesiophobia in individuals with CNLBP.
Another study [21] investigated the effect of PNE in a spinal manipulative therapy (SMT) protocol. The researchers hypothesised that a combination of SMT and PNE may improve pain in patients with CNLBP more than SMT alone. The trial involved 104 patients equally divided into two groups, with the first group (n = 52) following a SMT+PNE protocol and the second (n = 52) undergoing SMT alone. The SMT intervention included mobilisation techniques and spinal manipulation and was performed twice weekly for four weeks (eight treatments). The PNE programme contained only two 45-minute sessions carried out in conjunction with the first two SMT sessions. The PNE protocol helped patients understand the meaning of pain and how the human body reacts to it. The study evaluated pain intensity using the NPRS and low back pain disability with the ODI at baseline, after four weeks, and the first, third, and sixth months post-intervention. Secondary outcomes measured included the participant’s perceived effect of improvement using the Global Perceived Effect (GPE) scale, pain self-efficacy using the Pain Self-Efficacy Questionnaire (PSEQ), and fear avoidance beliefs through the Fear Avoidance Beliefs Questionnaire (FABQ). The results revealed insignificant improvement in both groups for all parameters after four weeks (p > 0.05). However, marked changes (p < 0.05) were found between groups at the three-month and six-month follow-ups, with the SMT+PNE group showing improvements over the SMT group. Corresponding results were also found for the ODI score at the six-month follow-up (p < 0.05). The researchers attributed these long-term effects to changes in secondary outcomes. More specifically, GPE and PSEQ improved in the SMT+PNE group compared to the SMT group after six months, leading the researchers to conclude that PNE contributed to better long-term pain management with significant medium-term benefits.
Saracoglu et al. [22]Turkey. Inclusion criteria were: age over 18 years, presenting with a primary complaint of LBP least 6 months, and being fluent in Turkish. Exclusion criteria included: prior spinal surgery, severe osteoporosis, cauda equina syndrome, lumbar stenosis, spinal fracture, malignancies, any systemic inflammatory disease other than LBP, and illiteracy. Thirty-five patients were randomized into two groups. The intervention group was given NPE and the control group was given traditional patient education (TPE studied the effect of PNE combined with MT on pain intensity and quality of life in CNLBP patients. They hypothesised that PNE with MT would contribute to further pain reduction and improved quality of life in people with CNLBP more than MT alone. The participants included 35 patients with CNLBP randomly divided into two groups (intervention and control). All participants followed the same MT programme involving eight 45-minute sessions over four weeks. In addition, the intervention group received PNE, which included learning about the ways in which pain intensity is affected by their thoughts and perceptions (one treatment per week, lasting 40-45 min), while the control group (n = 18) received information on lumbar anatomy, biomechanics, and function once before the first MT session. The NPRS and Short Form-36 questionnaire (SF-36) assessed pain intensity and quality of life, respectively, before and after the intervention. The results showed that the intervention and control groups had significant improvements in all variables in the fourth week compared to the initial measurement. However, the improvement was greater in terms of NPRS (p = 0.01) and SF-36 (p = 0.04) scores in the intervention group. The researchers concluded that the combination of MT and PNE was more effective at reducing pain and improving the quality of life of people with CNLBP.
Another trial [15] compared the efficacy of combining an MT protocol that included soft tissue mobilisation techniques (STMT) and PNE to STMT alone. The study included 28 CN- LBP patients randomly divided into two groups (intervention and control). All participants underwent four sessions of MT in the lumbar region twice a week for four weeks (eight treatments). The intervention group received two additional PNE sessions, one before starting and one after completing the MT programme. The content of the PNE training concerned perceptions of pain, the pain neuromatrix, and general mechanisms of pain induction and processing by the brain. Evaluations included the NPRS, the Central Sensitisation Inventory (CSI), the pressure pain threshold (PPT) assessment in the lumbar area using a digital algometer, the Pain Cata- strophising Scale (PCS), the TSK-17, and the Roland Morris Disability Questionnaire (K-RMDQ) at baseline and at four, six, and eight-week follow-up. The intervention group showed improvements in NPRS (p < 0.001), PPT (p < 0.001), RMDQ (p < 0.001), and TSK-17 (p < 0.001) at week four compared to corresponding control group values. These differences remained significant during the follow-up measurements. Consequently, the researchers concluded that combining PNE and MT had a positive effect on pain, low back pain disability, and psychological factors compared to MT alone.
In the clinical trial of Tellez-Garcia et al. [23], the short-term efficacy of combining a trigger point dry needling (TrP-DN) MT protocol with PNE was investigated in 12 CNLBP patients divided into two groups. The TrP-DN group received three sessions of dry needling in the gluteus medius and quadra- tus lumborum muscles over a week, while the TrP-DN+EDU group received PNE, which addressed their perceptions and beliefs about pain two to three times in the last two weeks of the intervention. The evaluation used the NPRS, RMDQ, ODI, TSK, and PPT, with the latter focusing on the C5-C6 zygapo- physeal joint, transverse process of the L3 vertebra, second metacarpal, and tibialis anterior muscle. Measurements were carried out before the intervention and one week after its completion. The results showed that participants in the TrP-DN+ EDU group had reduced rates of kinesiophobia (p = 0.008) and increased PPTs at L3 (p = 0.049) compared to the TrP-DN group. Both groups showed similar improvements in pain levels and disability, as well as PPTs at the C5-C6 zygapo- physeal joint. Furthermore, adding PNE to TrP-DN treatment in CNLBP patients appeared to play a significant role only in reducing kinesiophobia levels.
Discussion
Our review examined whether the addition of PNE can further improve the efficacy of an MT protocol in patients with CNLBP. The results showed that the efficacy of physiotherapy intervention increases when patients are trained in PNE in addition to MT techniques. Indeed, the studies showed reductions in pain intensity and low back pain disability [14, 15, 21, 22], patient quality of life improvement [22], as well as reductions in kinesiophobia and pressure sensitivity [23] with the addition of PNE despite the substantial heterogeneity between the MT protocols used (mobilisation - manipulation, soft tissue mobilisation techniques, and dry needling). The researchers pointed out that these positive effects may be due to a change in the way the patients manage their symptoms and a possible change in their attitude towards chronic pain.
Mt is a neurophysiological practice that includes, beyond the hands-on techniques, cognitive and contextual factors for dealing with pain [24-26]. In fact, research has shown that the analgesic effects of MT are due to neurophysiological changes in the activation of alpha motor neurons and autoimmune response systems and an increase in endorphins and serotonin in the blood, which occur throughout the nervous system [25]. However, MT techniques alone do not markedly reduce fear-avoidance, kinesiophobia, and catastrophising due to pain, causing a reduction in local pressure pain thresholds in patients with musculoskeletal pain [27, 28]. Hands-on techniques focus on the areas affected by symptoms (i.e., the local anatomical structures) and cannot directly affect more complex mechanisms involved in chronic pain, such as sensitisation or psychological and socioeconomic factors that are linked to the intensity and duration of the symptoms. On the other hand, research has shown that the single application of PNE does not produce long-term results if it is not combined with another treatment, such as therapeutic exercise [29].
An interpretation of MT protocol improvement after the addition of PNE is that the content of PNE training helped participants gain better awareness of the origin and severity of their pain, manage their negative emotions, and ultimately become more efficient in the long-term management of their symptoms. This conclusion was reached by Tavares et al. [21], who observed improvements three to six months post-intervention and attributed this delayed improvement to better self-management of symptoms. Therefore, it appears that MT and PNE complement each other when combined. Puente- dura and Flynn [9] agree and suggest that providing PNE within an MT context can enhance patient expectations in the rehabilitation process and refresh body schema within the brain.
The results of our work also agree with those of previous reviews, such as Clarke et al. [30], who concluded that combining MT and PNE could positively affect low back pain. However, the studies included in their review were of low quality, and the researchers highlighted the need for more investigation in the future.
Despite these promising findings, several potential biases could affect the interpretation of our results. Selection bias may have been introduced due to the inclusion criteria, which limited the review to studies published in English and those available in full text. Additionally, publication bias may be present since studies with significant findings are more likely to be published. Furthermore, there is a risk of performance bias as the studies varied widely in terms of the specific MT techniques and PNE content used, which may impact the gener- alisability of the results.
Another important consideration is the absence of unanticipated outcomes or side effect reporting, suggesting that either such issues were not observed or not reported. However, it is crucial to acknowledge that the lack of adverse event reporting does not necessarily indicate their absence and future studies should aim to provide more comprehensive reporting in this regard.
There were also some limitations to our review. Firstly, the heterogeneity among the studies posed a challenge to the synthesis of findings. Variations in study populations, such as age, gender, and baseline health status, may introduce inconsistencies in the reported outcomes and limit the generalis- ability of the findings. Additionally, the lack of standardised outcome measures across studies further complicates the comparison of results. Another notable limitation is the absence of studies directly comparing MT with other therapy techniques. This gap in the literature hinders our ability to assess the relative efficacy of MT compared to alternative interventions. In the future, more high-quality randomised controlled clinical trials investigating the efficacy of MT techniques with PNE in CNLBP patients should certainly be conducted to strengthen the relevance of the existing trials. Trials with a larger sample size and a longer intervention duration would give us more secure conclusions about the efficacy of this combination.
Conclusions
Physiotherapy intervention is more effective when, in addition to MT techniques, patients are educated about the neurophysiology of pain. Pain levels, functional disability, and kinesiophobia are reduced, while quality of life and patient’s ability to self-manage their pain improves. All studies showed that the combination of PNE and MT provided better results than individual interventions in patients with CNLBP.