Introduction
Trauma is one of the common indications for lower limb amputation in developing nations, while diabetes mellitus is more common in developed countries [1]. Globally, 57.7 million people had limbs amputated as a result of trauma in 2017. The most common traumatic causes of amputation of limbs were mechanical forces (10.4%), falls (36.2%), road traffic injuries (15.7%), and other transport-related injuries (11.2%) [2]. The injury burden of traumatic amputees is primarily borne by males, as they are considered more outgoing and more commonly road users compared to women [3]. Amputations are a significant cause of morbidity, and complications following them can delay rehabilitation and prosthesis application. A comprehensive rehabilitation protocol involving pain management, stump care, oedema control, positioning, exercise, prosthetic prescription, balance, gait training, and functional training is crucial for optimal prosthesis functional use [4, 5]. Successful prosthesis use after amputation necessitates physical and psychological rehabilitation and physiotherapy, and isokinetic muscle testing for precise muscular power definition, especially in young amputees [6, 7]. Isokinetic equipment offers accurate and reliable strength testing, even at low muscle power levels, due to its ability to produce maximum torque and to adapt the resistance to the patient’s effort, reducing injury risk. Furthermore, because the measuring device’s mechanism adapts the resistance to the patient’s effort, the isokinetic dynamometers are generally safe. The dynamometer in the isokinetic machine has the ability to adjust the resistance during the exercise as per the patient’s effort [8].
Immediate postoperative prosthesis (IPOP) facilitates early ambulation and shorter recovery by applying a soft, detachable dressing to patients’ residual limbs in the operating room using strapping techniques and composite materials, which allows for early gait training [9]. Gait training for amputees focuses on improving postural control and preventing abnormalities and complications like low back pain. The course includes training for finding the centre of gravity, bearing body weight on the prosthetic limb, balancing, and coping with environmental changes. To reduce the fall risk, parallel bars are incorporated. Transfemoral amputees have an asymmetric gait, with a broader stride on the prosthetic side and a shorter stance phase [10].
The Questionnaire for Persons with a Transfemoral Amputation (Q-TFA) is a new survey designed for younger people with a transfemoral amputation who use a socket-osseointegrated prosthesis, measuring their use, mobility, issues, and overall health, each scored separately from 0 to 100. The questionnaire consists of 70 questions, which require a duration of 20 min to fill out. The scoring system is divided into prosthetic use score, prosthetic mobility score, problem score, and global score [11].
Rehabilitation is an important pillar in the survival chain of a trauma victim, so the early rehabilitation of all patients is of utmost importance. The main objectives of postoperative care are stump preparation, oedema and pain control, and wound healing [12]. Treatment usually consists of a soft dressing and an elastic bandage. However, poorly wrapped elastic bandages frequently result in distal stump oedema. IPOP allows early prosthesis use, prevents joint flexion contracture, and protects the stump from injury. It enhances healing, helps amputees understand prosthesis components, provides economic and social benefits, enabling quicker social reintegration and shorter hospital stays [13]. Clinicians often use manual muscular testing for assessing patients’ strength but lack quantitative assessment. Isokinetic devices provide precise, reliable monitoring, even at limited potential ranges, and are safe due to their resistance adjustment mechanism [8]. The coordinated function of the muscles spanning the corresponding joints (ankles, knees, and hips) allows the lower extremities (foot, legs, and thighs) to move in synchrony during the human walk [14]. However, the unavoidable structural and functional alterations in the musculoskeletal system change the typical walking pattern after amputation. The ability to use a prosthetic limb is substantially correlated with quality of life after lower limb amputation. Above-knee amputees struggle to regain normal movement, requiring 80% more energy to walk than those with two legs due to knee movement complexities [15]. Trauma is the second most common cause of lower limb amputation, affecting young adults and men. Post-amputation complications delay prosthesis application and rehabilitation. A successful prosthesis necessitates both physical and psychological rehabilitation.
This study will be one of its kind on traumatic above-knee amputation patients, where an immediate postoperative pros-thesis will be provided to patients of both the isokinetic and conventional exercise groups. Muscle strengthening using an isokinetic dynamometer (Biodex system 4) will be unique since the system provides feedback to the patients. There is a dearth of literature on gait analysis in traumatic amputation patients, especially in the early phase post-amputation. The findings of the study will help in developing a protocol for early rehabilitation of above-knee amputation patients following trauma.
Objectives
The objectives of the study are to compare the effect of isokinetic versus conventional strength training exercises on above-knee amputation patients following trauma in relation to gait. The secondary objectives are acceptability of immediate postoperative prosthesis (IPOP) in relation to early stump preparation and assessment of quality-of-life parameters in above-knee amputation patients.
Subjects and methods
Patient and public involvement
Patients undergoing above-knee amputation following trauma at the Division of Trauma Surgery and Critical Care, level I trauma centre, will be enrolled in the study.
Trial design
This will be a randomised controlled trial and a type of non-inferiority trial in which a new treatment is not worse than an active (practicing) treatment, and a placebo cannot be used due to the institute’s standard of care for amputation patients.
Trial setting
Patients coming to the emergency department of the Division of Trauma Surgery and Critical Care trauma centre and being admitted to this trauma centre.
Eligibility criteria
Inclusion criteria
Exclusion criteria
– associated fractures of the extremity
– head or spine injury that hampers the mobility of the patient
– the patient requires ICU care for more than 24 h
– injuries due to which the patient cannot be mobilised, even 24 h after amputation
Patients in both groups will be advised to follow the standard care for amputees, which includes managing pain with medication, using high-frequency transcutaneous electrical nerve stimulation, at 80 Hz with a pulse width of 200 μs for 15 min using an Intelect advanced combo (Chattanooga, USA), applying cold therapy with a cold pack or with a Cryo-flow IR machine, and preparing the stump with a crepe bandage and shrinker, according to the institute’s guidelines.
Intervention
The participant will receive an isokinetic strength training exercise protocol after the application of an immediate postoperative prosthesis (Figure 1) and will be mobilised in the ward with the help of a walker under supervision. On the Biodex System 4 (Figure 2), the patient will be instructed to relax while the isokinetic dynamometer moves their limb at 60°/s through a range of 10° of hip extension to 70° of hip flexion. These steps will be repeated until the participant feels comfortable with their position and the movement. After instructing the participant to relax completely, we will collect the initial flexion and extension trials to determine the torque. Maximal concentric flexor and extensor strength measurements at 60°/s and 120°/s will be performed in random order with verbal encouragement throughout the entire range of motion. We will sample the output angle (degrees) and torque data (Nm) at 100 Hz [12]. The following protocol will be followed for the number of times the exercise is to be performed. In the first week, two sets with a rest period of 60 s will be done. For the slow movements, which are at 60°/s, the choice of a heavy weight that can be lifted 10 times in succession, and for the fast movements, which are at 120°/s, a lighter weight for 15 repetitions as fast as possible will be performed. In the second week, the same exercises will be repeated, but the number of sets will be three for both the slow and fast movements. The participants will receive isokinetic strength training 5 times a week over the period of 2 weeks.


Control: Participants in this group will do the conventional exercise training protocol 5 times a week over the duration of 2 weeks. The exercise protocol is outlined in detail below:
– limb lifts: lying on back (hip flexion)
– limb press (hip extension)
– limb slides (hip abduction and adduction)
– hip strengthening (isometric hip abduction and adduction)
– thigh stretch (hip flexor stretch) – buttocks squeeze (gluteal sets)
– single-leg bridge on full leg (unilateral hip extension bridge)
– limb lifts: lying on your side (side-lying hip abduction)
– limb lifts: lying on stomach (prone hip extension)
– chair push-ups (triceps push-ups)
All the above-mentioned exercises will be done under supervision using manual resistance. Two sets of 10 repetitions will be done in the first week, and this will be increased to three sets of 10 repetitions in the second week. Exercises will be monitored and supervised with an equal number of repetitions and the duration to be kept the same for patients in both groups to maintain uniformity. Along with this, balance and gait training, mobilising, and putting on and taking off the IPOP will be taught to the patients in both groups. Patients will also receive psychological support to improve treatment compliance. A psychiatrist and a psychologist are involved in the current trial, and all the patients will be regularly evaluated by them for any psychosocial issues.
Once the exercise training in both groups is terminated, which is at two weeks, the strength of the hip muscles (flex-ors, extensors, and abductors) will be measured using a Biodex System 4 for both groups. The Biodex System 4 will determine the average peak torque. The protocol to be used to measure the strength of the hip muscles will be two trials of 10 repetitions at 60°/s and 120°/s with a 30 s rest period [16].
Outcomes
Primary outcome
All the patients will be assessed on the following outcome at three time points: 2 weeks, 6 weeks and 12 weeks from the day of amputation.
– Strength of hip muscles using the Biodex system 4
– Q-TFA (Questionnaire for Persons with Transfemoral Amputation) psychological scale as per the attached proforma, which is a self-administered scale
– Gait analysis for biomechanical motion analysis using the BTS Smart-DX
The first assessment will be done at the second week mark after completing exercise training of 10 sessions for hip muscle strength and Q-TFA. Follow-up assessments will be done at 6 and 12 weeks for hip muscle strength, Q-TFA and gait analysis.
Secondary outcomes
They include calculation of stump-ready status, for which stump maturation evaluation will be performed. The patients will be provided with a definitive prosthesis once the stump is matured using the Clinical Standard of Measurement and Classification of Amputation Stumps ISPO 1982 [17]. They will also be evaluated for the number of hours they wear the prosthesis each day.
Definitive prosthesis and gait analysis
With respect to definitive prosthesis application, it is our practice to advise prosthesis to all amputees between 4 and 6 weeks after amputation, since that much time is needed for stump maturation. However, for the purpose of this study, both the IPOP and definitive prosthesis will be provided to all the patients free of cost from the funds received via an extramural grant.
Gait analysis parameters
Patients will be called into the gait lab (Figure 3) available at the Institute with prior appointment and will be assessed at 6 and 12 weeks. The modified Helen Hayes protocol will be used for marker placement [18]. Eighteen reflective markers are used as per this protocol, with the placement being three on the trunk (C7, right and left acromion), three on the pelvis (S2, right and left ASIS), four on the thigh (right and left thigh in line with the greater trochanter, right and left lateral femoral condyle), four on the shank (right and left malleolus, right and left shank), and four on the foot (in between the 2nd and 3rd metatarsal on both sides, right and left heel). Double-sided sticky tape will be used to secure the markers on the patient’s body. These reflective marker locations are tracked by infrared cameras to facilitate 3D reconstruction.

Three sets of parameters will be evaluated at the gait lab: (1) Temporal and spatial parameters: mean velocity (m/s) which measures speed, cadence (steps/min), double support phase (%) and step width (cm). (2) Kinematic parameters: pelvic obliquity, peak hip flexion, peak knee flexion, and hip abduction. (3) Kinetic parameters: hip power (W/kg) and anterior propulsion ground reaction force (% body weight).
Harms
Although the intervention, which is isokinetic training, is generally safe to use, some risks are still present, which include muscle strain from overexertion. To overcome such harms, monitored exercises will be performed for the patients in both groups.
Participant timeline
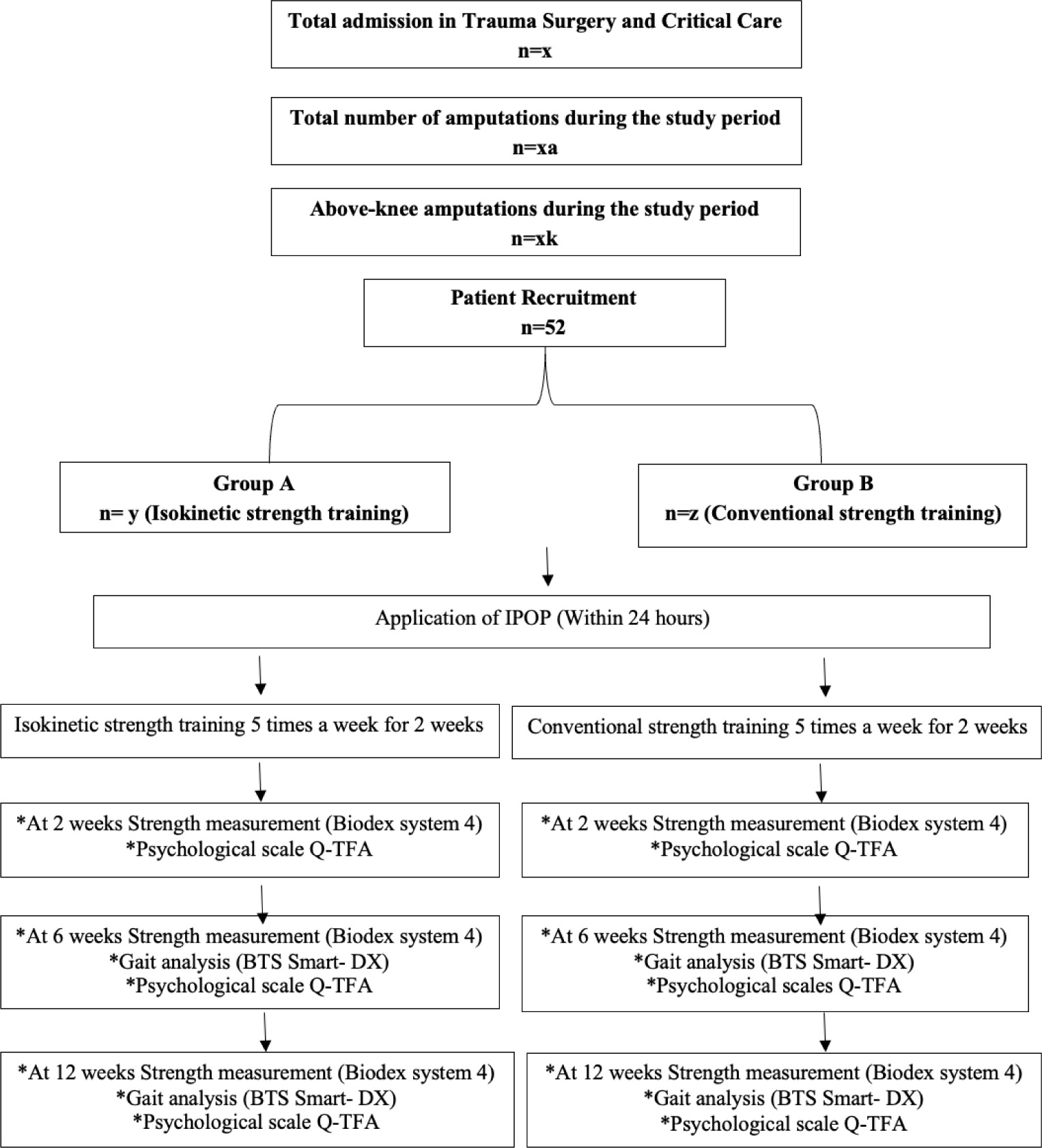
Participants will be enrolled in the study for the duration of 12 weeks following amputation. They will be assessed at three time points, which are at 2 weeks, 6 weeks and 12 weeks following amputation. The same is depicted in Figure 4.
Sample size
We will enrol patients who meet the inclusion criteria in the study after obtaining their informed consent. We will recruit patients with above-knee amputation following trauma for this interventional study. With an expectation of a 15% change in the improvement in gait pattern at 6 weeks and a 10% loss to follow-up at 80% power of the study, the calculated or expected sample size is 52 (26 in each arm).
Recruitment
All patients who will be received in the emergency department of the trauma centre undergoing above-knee amputation will be assessed for eligibility to enrol in the study. Patients who fulfil the inclusion criteria and give consent to participate in the study will be enrolled.
Random sequence generation: A computer-generated allocation of sequentially numbered envelopes having a block size of 4 will be created by the PhD student implementing this research.
Allocation concealment mechanism
These envelopes will be kept in a sealed, opaque envelope in the office of the chief guide. Patients will be randomised into two groups. The envelope will be opened by the office staff of the chief guide and conveyed to the PhD student.
Implementation
The enrolment, intervention, and outcome assessment will be done by the PhD student. This work is the thesis work of this PhD candidate.
Blinding
The participants of each group will be blinded about the type of exercises the other group will be doing. There is no significant need to blind the outcome assessors since the outcome is objective measurements using the Biodex system 4 and BTS Smart-DX, and one psychological scale is used, which is a self-administered scale where the participants will fill out the questionnaire on their own.
Data collection methods
Data will be collected and maintained both in hard copy and as an Excel spreadsheet, which will be kept in the office of the chief guide. Outcomes will be assessed by the PhD student herself on the Biodex and in the gait lab. One outcome measure is a self-administered questionnaire that will be available in both English and Hindi languages and will be filled out by the patients themselves. The data will be secured in the office of the chief guide and the confidentiality of the data will be maintained.
Data management
The data related to the questionnaire will be filled out as a hard copy, and data generated from the Biodex system and gait will be received in the form of reports, and later, all the data will be entered in the Excel spreadsheet. The data will be monitored by the chief guide.
Data monitoring committee
The doctoral committee, comprising experts from the fields of surgery, orthopaedics and physiotherapy, team members of the special amputation clinic, has been formed for the PhD candidate, who will take on the responsibility of data monitoring.
Trial monitoring
As per the Institute’s protocol, it is mandatory to monitor the work of the PhD candidate every six months. A doctoral committee meeting will be planned every six months or in between in case of any need to monitor the trial and its progression.
Data sharing
All the data, including de-identified proforma case records, assessment sheets and other records of the patients, will be kept in the office of the chief guide. Data will be stored for 5 years after the completion of the study and will be shared on reasonable request to the corresponding author.
Open science
Protocol and statistical analysis plan: Data will be collected in printed and electronic format using Excel version 2021. Descriptive statistics will be used to present the data. Qualitative data will be presented in absolute numbers and percentages. Quantitative data will be assessed for normality. If the normality of the data is confirmed, the means with standard deviations will be reported, and if not, the medians with interquartile ranges.
To establish the association between the outcome and exposure variables, the chi-square / Fisher’s exact test will be used. To observe the change between outcomes, the independent t-test will be used if the data distribution is normal, and the Wilcoxon rank-sum test if it is not. All data will be assessed for missing observations, and if required, imputation will be performed. A per-protocol and intention-to-treat analysis will be performed wherever required. A p-value of less than 0.05 will be considered statistically significant. All the data will be analysed with the help of STATA MP version 18.
The SPIRIT 2025 checklist is followed for reporting a clinical trial protocol.
Dissemination policy: The investigators plan to disseminate the trial results to researchers and clinicians addressing amputee rehabilitation. The findings of the study will also aid in preparing guidelines for early rehabilitation of traumatic above-knee amputation patients.